

A European Multicenter Outcome Study of Perioperative Airway Management Policies following Midface Surgery in Syndromic Craniosynostosis
- PMID: 38289904
- PMCID: PMC11584185
- DOI: 10.1097/PRS.0000000000011317
A European Multicenter Outcome Study of Perioperative Airway Management Policies following Midface Surgery in Syndromic Craniosynostosis
Abstract
Background: Perioperative airway management following midface advancements in children with Apert and Crouzon-Pfeiffer syndromes can be challenging, and protocols often differ. This study examined airway management following midface advancements and postoperative respiratory complications.
Methods: A multicenter, retrospective cohort study was performed to obtain information about the timing of extubation, perioperative airway management, and respiratory complications after monobloc or Le Fort III procedures.
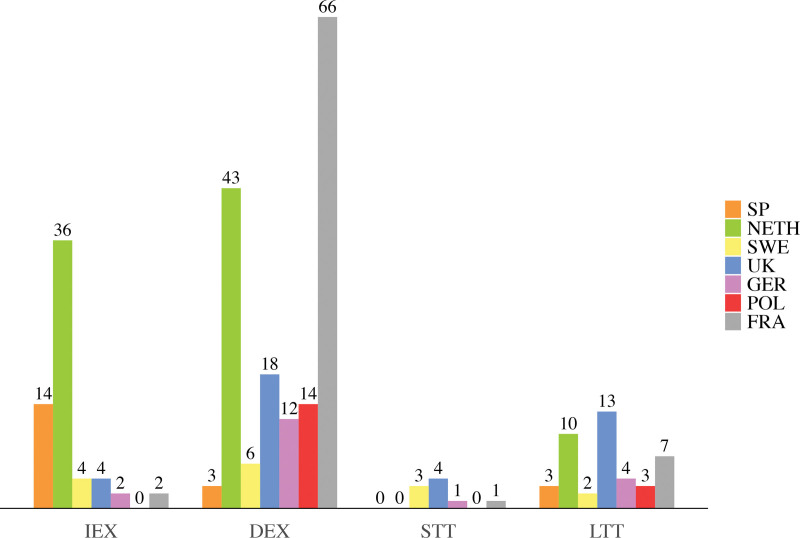
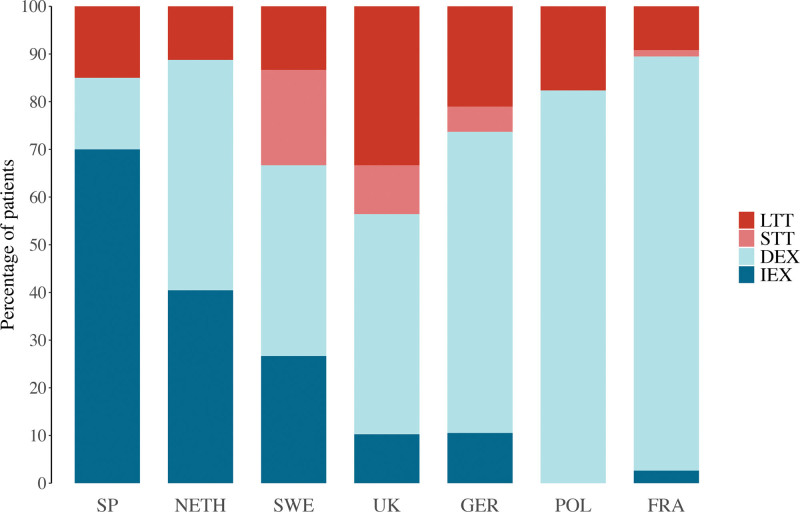
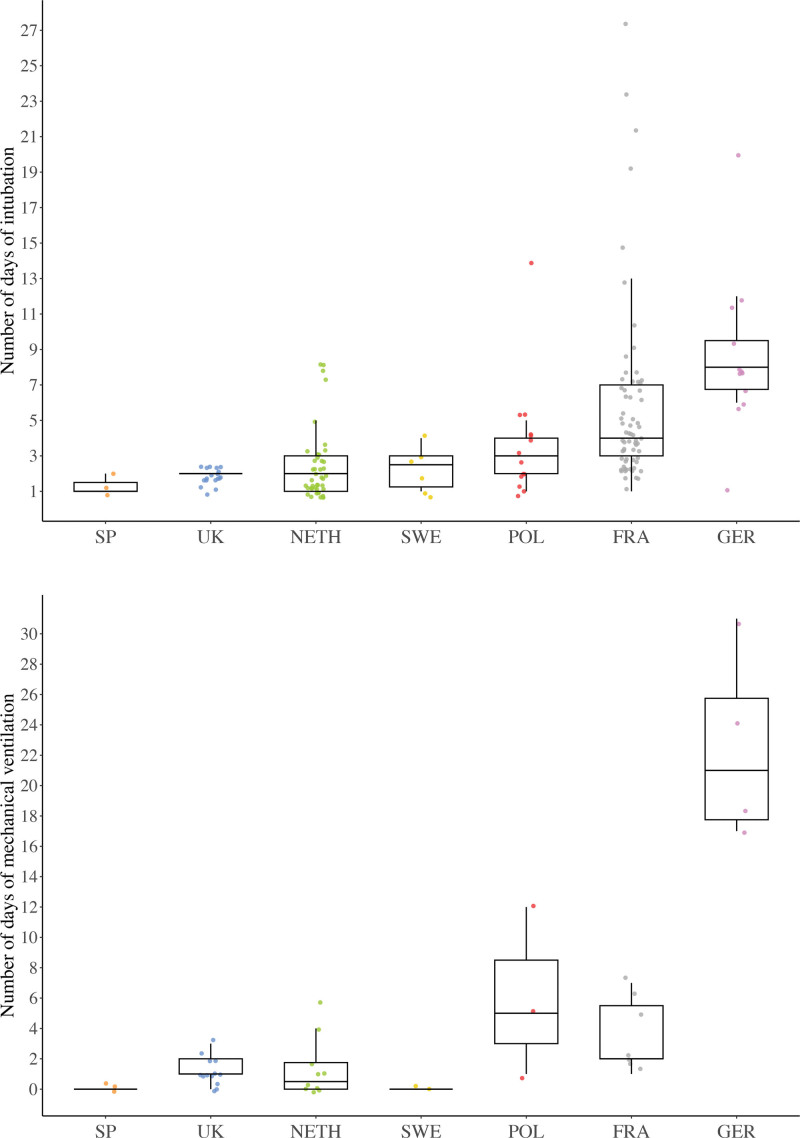
Results: A total of 275 patients (monobloc surgery, n = 129; Le Fort III surgery, n = 146) were included. Sixty-two patients received immediate extubation and 162 received delayed extubation; 42 had long-term tracheostomies, and 9 had perioperative short-term tracheostomies. In most centers, short-term tracheostomies were reserved for selected cases. Patients with delayed extubation remained intubated for 3 days (interquartile range, 2 to 5 days). The rate of no or only oxygen support after extubation was comparable between immediate and delayed extubation groups (58 of 62 patients [94%] and 137 of 162 patients [85%], respectively). However, the immediate extubation group developed fewer cases of postoperative pneumonia than did the delayed group (0 of 62 [0%] versus 24 of 161 [15%]; P = 0.001). Immediate extubation also appeared safe in moderate to severe obstructive sleep apnea, as 19 of 20 patients (95%) required either no or only oxygen support after extubation. The odds of developing intubation-related complications increased by 21% with every extra day of intubation.
Conclusions: Immediate extubation following midface advancements was found to be a safe option, as it was not associated with respiratory insufficiency but did lead to fewer complications. Immediate extubation should be considered routine management in patients with no or mild obstructive sleep apnea, and should be the aim in moderate to severe obstructive sleep apnea cases after careful assessment.
Clinical question/level of evidence: Therapeutic, III.
Copyright © 2024 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of the American Society of Plastic Surgeons.
Conflict of interest statement
The authors have no conflicts of interest to report.
Figures
References
-
- Driessen C, Joosten KF, Bannink N, et al. . How does obstructive sleep apnoea evolve in syndromic craniosynostosis? A prospective cohort study. Arch Dis Child. 2013;98:538–543. - PubMed
-
- Elmi P, Reitsma JH, Buschang PH, Wolvius EB, Ongkosuwito EM. Mandibular asymmetry in patients with the Crouzon or Apert syndrome. Cleft Palate Craniofac J. 2015;52:327–335. - PubMed
-
- Hoeve HL, Joosten KF, van den Berg S. Management of obstructive sleep apnea syndrome in children with craniofacial malformation. Int J Pediatr Otorhinolaryngol. 1999;49:S59–S61. - PubMed
-
- Kim JH, Guilleminault C. The nasomaxillary complex, the mandible, and sleep-disordered breathing. Sleep Breath. 2011;15:185–193. - PubMed
-
- Lo LJ, Chen YR. Airway obstruction in severe syndromic craniosynostosis. Ann Plast Surg. 1999;43:258–264. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
