

Single-cell analysis of refractory anti-SRP necrotizing myopathy treated with anti-BCMA CAR-T cell therapy
- PMID: 38289960
- PMCID: PMC10861907
- DOI: 10.1073/pnas.2315990121
Single-cell analysis of refractory anti-SRP necrotizing myopathy treated with anti-BCMA CAR-T cell therapy
Abstract
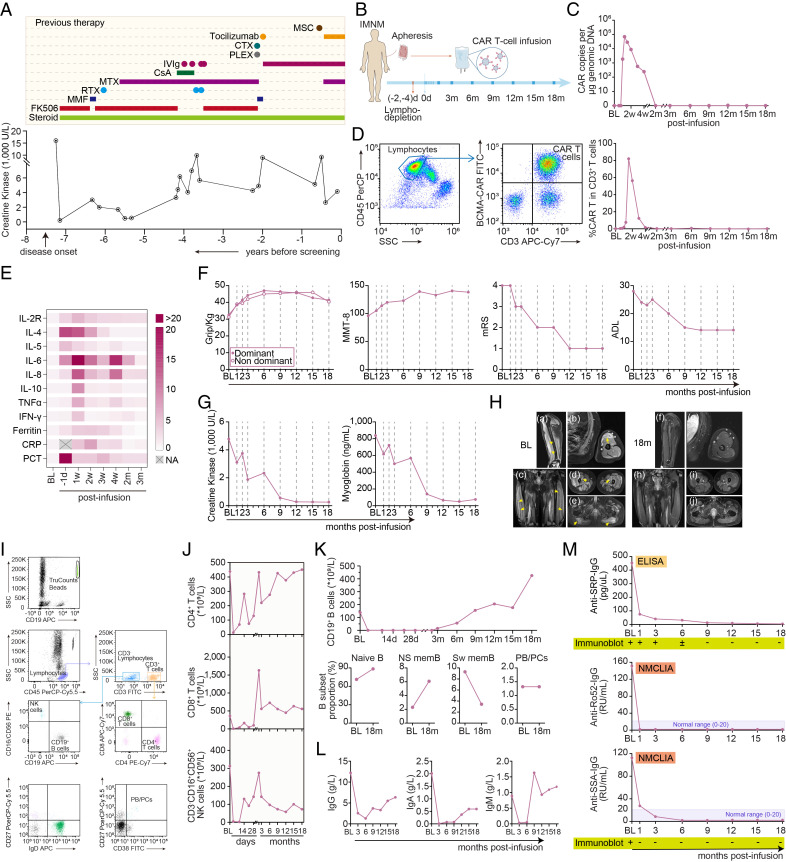
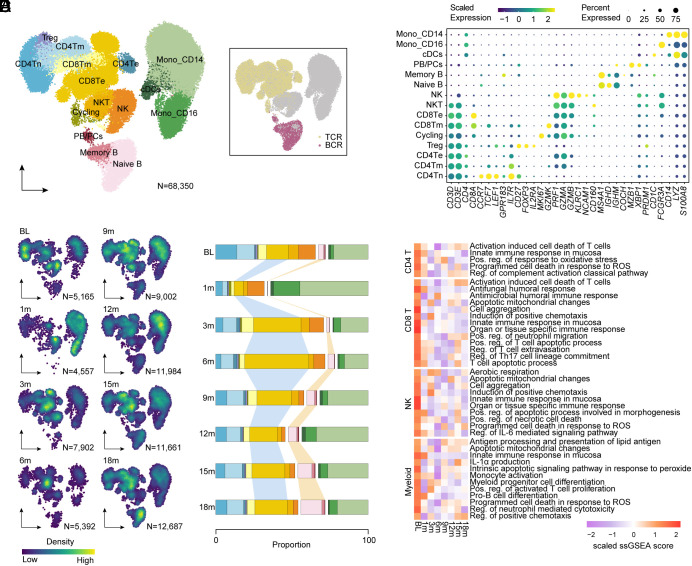
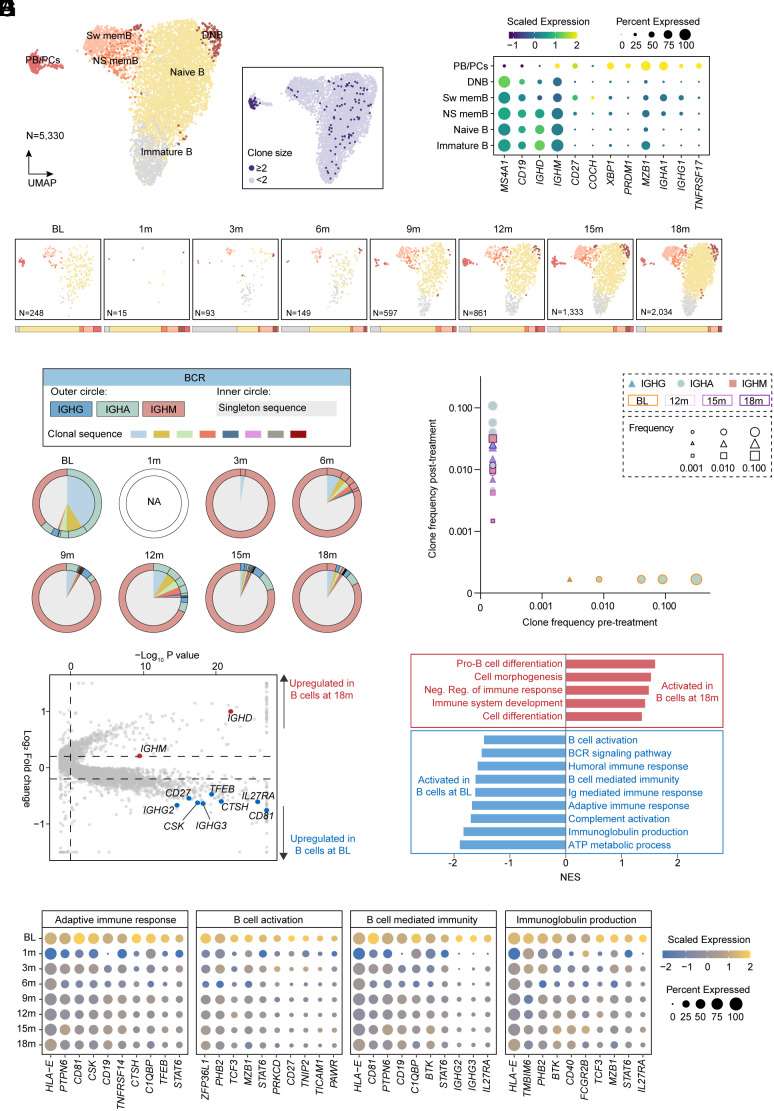
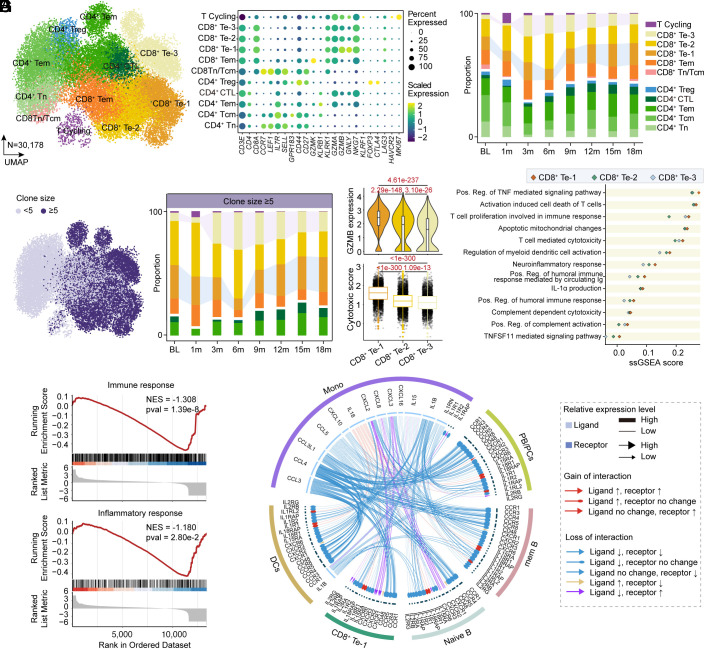
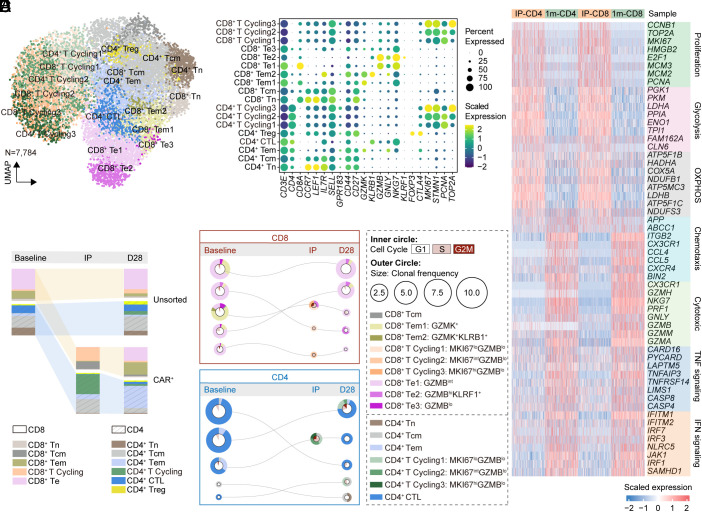
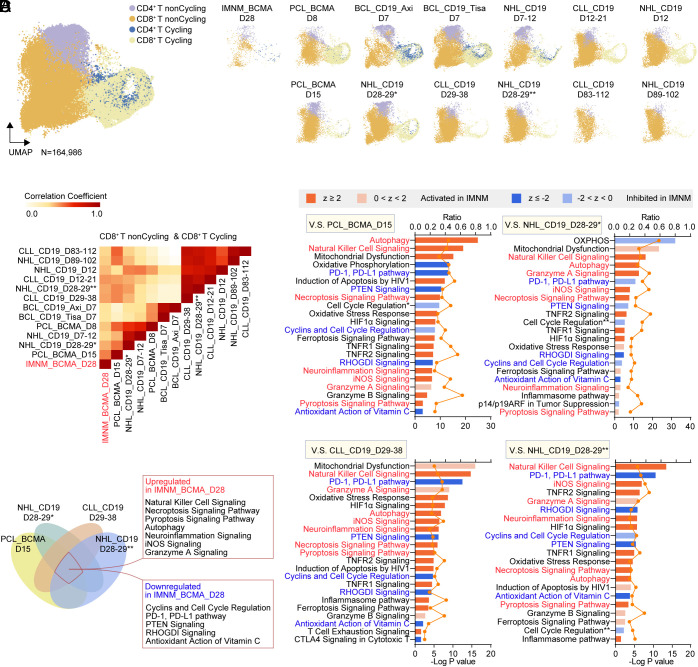
Immune-mediated necrotizing myopathy (IMNM) is an autoimmune disorder associated with the presence of autoantibodies, characterized by severe clinical presentation with rapidly progressive muscular weakness and elevated levels of creatine kinase, while traditional pharmacological approaches possess varying and often limited effects. Considering the pathogenic role of autoantibodies, chimeric antigen receptor (CAR)-T cells targeting B cell maturation antigen (BCMA) have emerged as a promising therapeutic strategy. We reported here a patient with anti-signal recognition particle IMNM refractory to multiple available therapies, who was treated with BCMA-targeting CAR-T cells, exhibited favorable safety profiles, sustained reduction in pathogenic autoantibodies, and persistent clinical improvements over 18 mo. Longitudinal single-cell RNA, B cell receptor, T cell receptor sequencing analysis presented the normalization of immune microenvironment after CAR-T cell infusion, including reconstitution of B cell lineages, replacement of T cell subclusters, and suppression of overactivated immune cells. Analysis on characteristics of CAR-T cells in IMNM demonstrated a more active expansion of CD8+ CAR-T cells, with a dynamic phenotype shifting pattern similar in CD4+ and CD8+ CAR-T cells. A comparison of CD8+ CAR-T cells in patients with IMNM and those with malignancies collected at different timepoints revealed a more NK-like phenotype with enhanced tendency of cell death and neuroinflammation and inhibited proliferating ability of CD8+ CAR-T cells in IMNM while neuroinflammation might be the distinct characteristics. Further studies are warranted to define the molecular features of CAR-T cells in autoimmunity and to seek higher efficiency and longer persistence of CAR-T cells in treating autoimmune disorders.
Keywords: B cell maturation antigen; chimeric antigen receptor (CAR) T cell; immune mediated necrotizing myopathy; single-cell RNA sequencing.
Conflict of interest statement
Competing interests statement:Wen Wang and S.-B.C. are employees of Nanjing IASO Therapeutics Ltd. and held interests in the company. Wen Wang held interests in patent applications related to the CT103A. All other authors declare no competing interest.
Figures
References
-
- Allenbach Y., Mammen A. L., Benveniste O., Stenzel W., Immune-mediated necrotizing myopathies working G 224th ENMC International Workshop: Clinico-sero-pathological classification of immune-mediated necrotizing myopathies Zandvoort, The Netherlands, 14–16 October 2016. Neuromuscul. Disord. 28, 87–99 (2018). - PubMed
-
- Anquetil C., Boyer O., Wesner N., Benveniste O., Allenbach Y., Myositis-specific autoantibodies, a cornerstone in immune-mediated necrotizing myopathy. Autoimmun. Rev. 18, 223–230 (2019). - PubMed
-
- Day J. A., Limaye V., Immune-mediated necrotising myopathy: A critical review of current concepts. Semin. Arthritis. Rheum. 49, 420–429 (2019). - PubMed
-
- Baker D. J., June C. H., CAR T therapy extends its reach to autoimmune diseases. Cell 185, 4471–4473 (2022). - PubMed
MeSH terms
Substances
Grants and funding
- 2022ZD0204700/Ministry of Sciences and Technology China Brain Initiative Grant STI2030-Major Projects
- 82071380/MOST | National Natural Science Foundation of China (NSFC)
- 82271341/MOST | National Natural Science Foundation of China (NSFC)
- 2022020801020454/Knowledge Innovation Program of Wuhan Shuguang Project
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
