

Association between antithrombotic therapy after stroke in patients with atrial fibrillation and the risk of net clinical outcome: an observational cohort study
- PMID: 38290433
- PMCID: PMC10872674
- DOI: 10.1093/europace/euae033
Association between antithrombotic therapy after stroke in patients with atrial fibrillation and the risk of net clinical outcome: an observational cohort study
Abstract
Aims: Data on the optimal use of antithrombotic drugs and associated clinical outcomes in patients with atrial fibrillation (AF) and acute ischaemic stroke (IS) are limited. We investigated the prescription patterns of antithrombotics in community practice and long-term clinical prognosis according to early post-stroke antithrombotic therapy in patients with AF and acute IS.
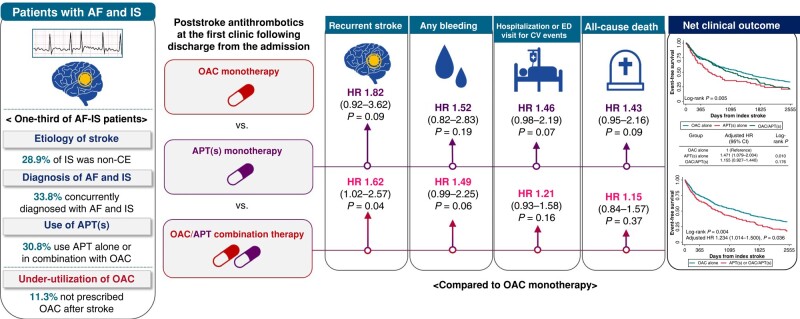
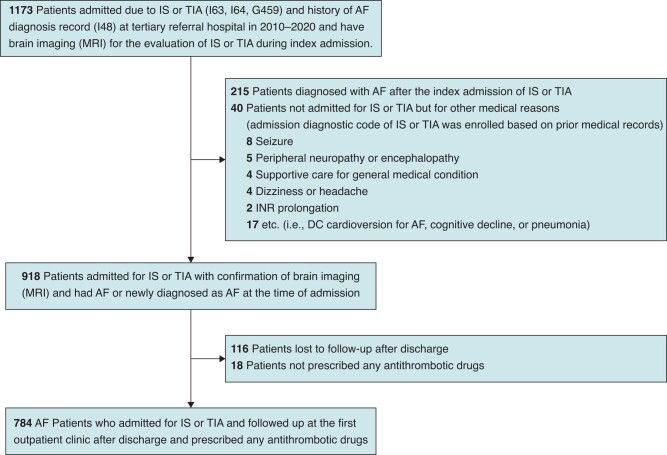
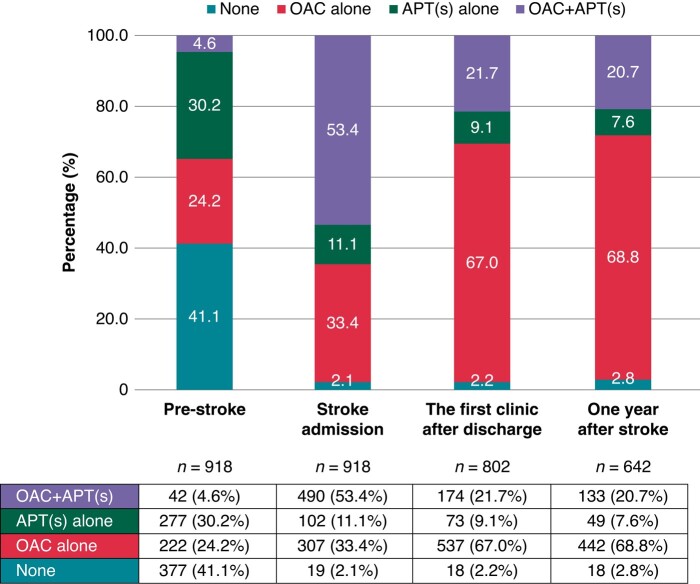
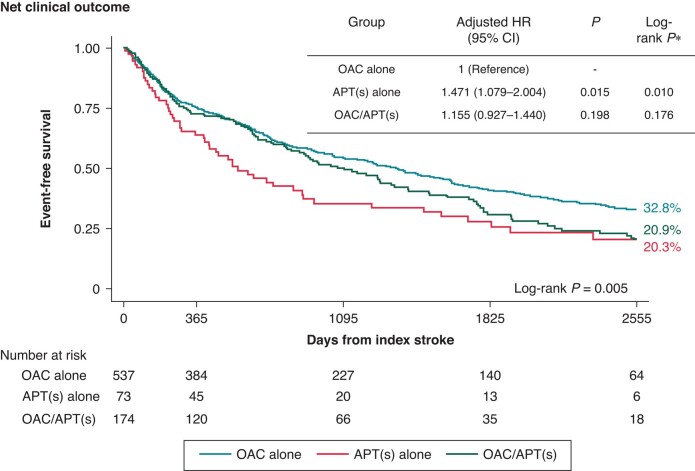
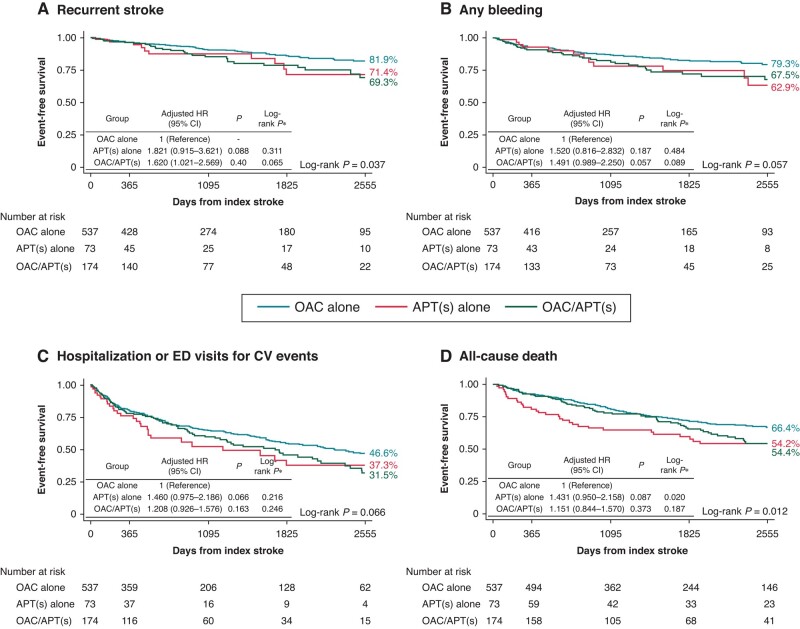
Methods and results: Patients with AF who were admitted for acute IS at a single tertiary hospital in 2010-2020 were retrospectively reviewed. Clinical profiles including the aetiology of stroke and prescription patterns of antithrombotics were identified. The net clinical outcome (NCO)-the composite of recurrent stroke, any bleeding, hospitalization or emergency department visits for cardiovascular (CV) events, and death-was compared according to the antithrombotic therapy at the first outpatient clinic visit [oral anticoagulation (OAC) alone vs. antiplatelet (APT) alone vs. OAC/APT(s)] following discharge. A total of 918 patients with AF and acute IS (mean age, 72.6 years; male, 59.3%; mean CHA₂DS₂-VASc score 3.3) were analysed. One-third (33.9%, n = 310) of patients were simultaneously diagnosed with AF and IS. The most common aetiology of IS was cardioembolism (71.2%), followed by undetermined aetiology (19.8%) and large artery atherosclerosis (6.0%). OAC, APT(s), and concomitant OAC and APT(s) were prescribed in 33.4%, 11.1%, and 53.4% of patients during admission that changed to 67.0%, 9.1%, and 21.7% at the first outpatient clinic, and were mostly continued up to one year after IS. Non-prescription of OAC was observed in 11.3% of post-stroke patients with AF. During a median follow-up of 2.1 years, the overall incidence rate of NCO per 100 patient-year (PY) was 20.14. APT(s) monotherapy presented the highest cumulative risk of NCO (adjusted hazard ratio 1.47, 95% confidence interval 1.08-2.00, P = 0.015; with reference to OAC monotherapy) mainly driven by the highest rates of recurrent stroke and any bleeding. OAC/APT(s) combination therapy was associated with a 1.62-fold significantly higher risk of recurrent stroke (P = 0.040) and marginally higher risk of any bleeding than OAC monotherapy.
Conclusion: Approximately one-third of acute IS in AF have a distinctive mechanism from cardioembolism. Although APT was frequently prescribed in post-stroke patients with AF, no additive clinical benefit was observed. Adherence to OAC treatment is essential to prevent further CV adverse events in patients with AF and IS.
Keywords: Antiplatelet; Antithrombotics; Atrial fibrillation; Ischaemic stroke; Oral anticoagulation.
© The Author(s) 2024. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: H.-J.A., J.M.C., K.-Y.L., S.K., S.O.: none. S.-R.L.: speaking fees from Bayer, BMS/Pfizer, Biosense Webster, Daiichi-Sankyo, Sanofi-Aventis, Daewoong Pharmaceutical Co., Samjinpharm, Seers Technology, Biotronik, Boston Scientific, and Medtronic. Consultant for Biosense Webster. No fees are received personally and no fees are related to this work. E.-K.C.: research grants or speaking fees from Abbott, Bayer, BMS/Pfizer, Biosense Webster, Chong Kun Dang, Daewoong Pharmaceutical Co., Daiichi-Sankyo, DeepQure, Dreamtech Co., Ltd., Jeil Pharmaceutical Co. Ltd, Medtronic, Samjinpharm, Seers Technology, and Skylabs. G.Y.H.L.: consultant and speaker for BMS/Pfizer, Boehringer Ingelheim, Anthos, and Daiichi-Sankyo. No fees are received personally. G.Y.H.L. is co-principal investigator of the AFFIRMO project on multimorbidity in AF, which has received funding from the European Union’s Horizon 2020 research and innovation programme under grant agreement no. 899871.
Figures
References
-
- Lip GY, Lane DA. Stroke prevention in atrial fibrillation: a systematic review. JAMA 2015;313:1950–62. - PubMed
-
- Kleindorfer DO, Towfighi A, Chaturvedi S, Cockroft KM, Gutierrez J, Lombardi-Hill Det al. . 2021 guideline for the prevention of stroke in patients with stroke and transient ischemic attack: a guideline from the American Heart Association/American Stroke Association. Stroke 2021;52:e364–467. - PubMed
-
- Evans A, Perez I, Yu G, Kalra L. Should stroke subtype influence anticoagulation decisions to prevent recurrence in stroke patients with atrial fibrillation? Stroke 2001;32:2828–32. - PubMed
-
- Klijn CJ, Paciaroni M, Berge E, Korompoki E, Korv J, Lal Aet al. . Antithrombotic treatment for secondary prevention of stroke and other thromboembolic events in patients with stroke or transient ischemic attack and non-valvular atrial fibrillation: a European Stroke Organisation guideline. Eur Stroke J 2019;4:198–223. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
