

Comprehensive treatment protocol for peri-implantitis: an up-to date narrative review of the literature
- PMID: 38290998
- PMCID: PMC11543328
- DOI: 10.5051/jpis.2303360168
Comprehensive treatment protocol for peri-implantitis: an up-to date narrative review of the literature
Abstract
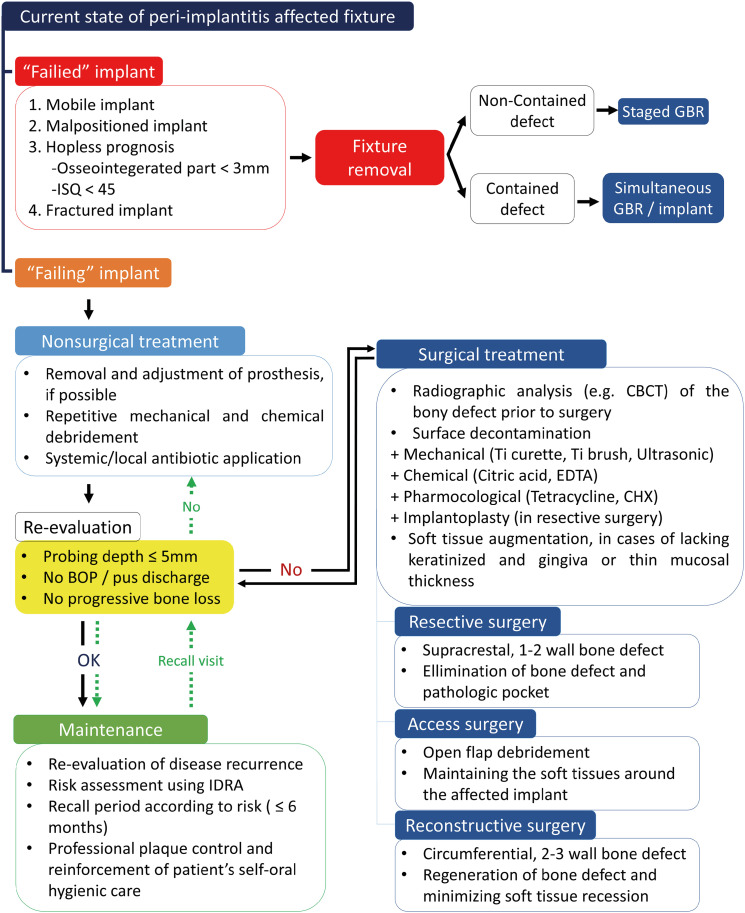
This narrative review describes up-to-date treatment options for peri-implantitis and proposes a treatment protocol and flowchart based on the current scientific evidence. Peri-implantitis treatment should be based on the phased treatment protocol for periodontitis, which is a continuous flow of decisions for extraction, nonsurgical and surgical treatments with step-by-step re-evaluation. The protocol's goals are to fulfill the success criteria for peri-implantitis treatment (probing depth of ≤5 mm, and absence of bleeding on probing, suppuration, and progressive bone loss) and to halt disease progression. Fixtures with peri-implantitis can initially be classified as failed or failing. A failed implant needs to be removed. In contrast, nonsurgical and surgical treatments can be applied to a failing implant. Nonsurgical treatment should be the initial treatment for failing implants; however, sole nonsurgical treatment was regarded as inefficient for peri-implantitis. Recent studies have found that the adjunctive use of antibiotics to nonsurgical debridement increased the success of nonsurgical treatment for peri-implantitis. Surgical treatments can be classified into resective, access, and reconstructive surgeries. The technique should be selected according to the patient's bone defect configuration, which relate to regenerative potential. Various combinations of decontamination methods (e.g., mechanical, chemical, and pharmacological approaches) are required to achieve absolute surface decontamination. Clinicians should select an appropriate surface decontamination strategy according to the purpose of surgery. After signs of disease disappear and its progression is halted through active peri-implantitis treatment, it is necessary to enroll patients into maintenance programs. Compliance of patients with the maintenance program reduces the recurrence of peri-implantitis and sustains clinical success after treatment. Maintenance visits should include professional plaque control and hygiene care reinforcement for patients, and their interval should be set according to individual peri-implantitis risk. Clinicians should remind that peri-implantitis treatment is not a single procedure, but rather a continuing cycle of treatment and re-evaluation.
Keywords: Clinical protocols; Dental implants; Flowchart; Peri-implantitis.
Copyright © 2024. Korean Academy of Periodontology.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
References
-
- Berglundh T, Armitage G, Araujo MG, Avila-Ortiz G, Blanco J, Camargo PM, et al. Peri-implant diseases and conditions: consensus report of workgroup 4 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J Clin Periodontol. 2018;45(Suppl 1):S286–S291. - PubMed
-
- Derks J, Schaller D, Håkansson J, Wennström JL, Tomasi C, Berglundh T. Effectiveness of implant therapy analyzed in a swedish population: prevalence of peri-implantitis. J Dent Res. 2016;95:43–49. - PubMed
-
- Derks J, Schaller D, Håkansson J, Wennström JL, Tomasi C, Berglundh T. Peri-implantitis - onset and pattern of progression. J Clin Periodontol. 2016;43:383–388. - PubMed
-
- Araujo MG, Lindhe J. Peri-implant health. J Periodontol. 2018;89(Suppl 1):S249–S256. - PubMed
-
- Carcuac O, Abrahamsson I, Albouy JP, Linder E, Larsson L, Berglundh T. Experimental periodontitis and peri-implantitis in dogs. Clin Oral Implants Res. 2013;24:363–371. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
