

Mismatch between subjective and objective dysautonomia
- PMID: 38291116
- PMCID: PMC10828385
- DOI: 10.1038/s41598-024-52368-x
Mismatch between subjective and objective dysautonomia
Abstract
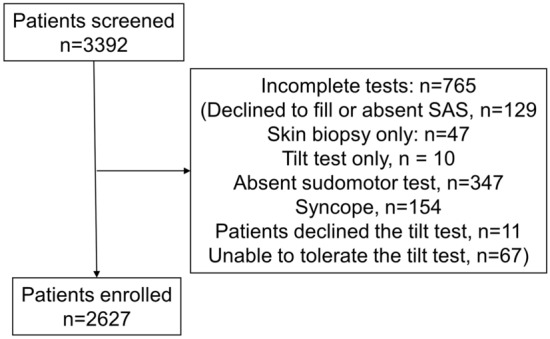
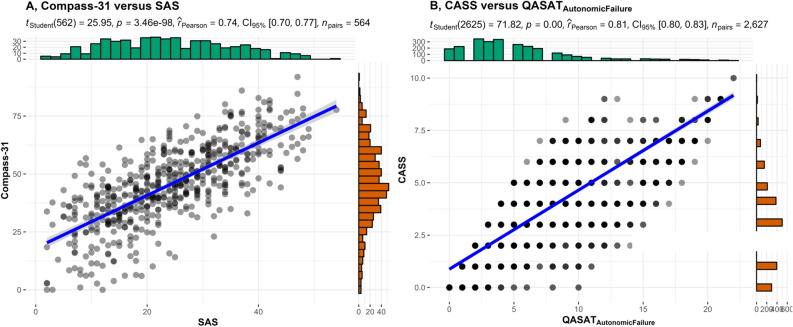
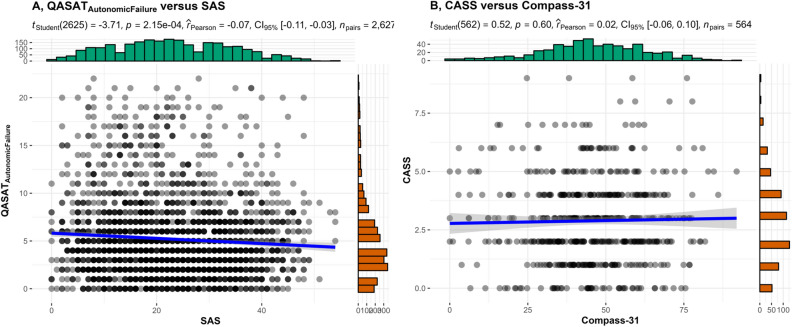
Autonomic symptom questionnaires are frequently used to assess dysautonomia. It is unknown whether subjective dysautonomia obtained from autonomic questionnaires correlates with objective dysautonomia measured by quantitative autonomic testing. The objective of our study was to determine correlations between subjective and objective measures of dysautonomia. This was a retrospective cross-sectional study conducted at Brigham and Women's Faulkner Hospital Autonomic Laboratory between 2017 and 2023 evaluating the patients who completed autonomic testing. Analyses included validated autonomic questionnaires [Survey of Autonomic Symptoms (SAS), Composite Autonomic Symptom Score 31 (Compass-31)] and standardized autonomic tests (Valsalva maneuver, deep breathing, sudomotor, and tilt test). The autonomic testing results were graded by a Quantitative scale for grading of cardiovascular reflexes, sudomotor tests and skin biopsies (QASAT), and Composite Autonomic Severity Score (CASS). Autonomic testing, QASAT, CASS, and SAS were obtained in 2627 patients, and Compass-31 in 564 patients. The correlation was strong between subjective instruments (SAS vs. Compass-31, r = 0.74, p < 0.001) and between objective instruments (QASAT vs. CASS, r = 0.81, p < 0.001). There were no correlations between SAS and QASAT nor between Compass-31 and CASS. There continued to be no correlations between subjective and objective instruments for selected diagnoses (post-acute sequelae of COVID-19, n = 61; postural tachycardia syndrome, 211; peripheral autonomic neuropathy, 463; myalgic encephalomyelitis/chronic fatigue syndrome, 95; preload failure, 120; post-treatment Lyme disease syndrome, 163; hypermobile Ehlers-Danlos syndrome, 213; neurogenic orthostatic hypotension, 86; diabetes type II, 71, mast cell activation syndrome, 172; hereditary alpha tryptasemia, 45). The lack of correlation between subjective and objective instruments highlights the limitations of the commonly used questionnaires with some patients overestimating and some underestimating true autonomic deficit. The diagnosis-independent subjective-objective mismatch further signifies the unmet need for reliable screening surveys. Patients who overestimate the symptom burden may represent a population with idiosyncratic autonomic-like symptomatology, which needs further study. At this time, the use of autonomic questionnaires as a replacement of autonomic testing cannot be recommended.
© 2024. The Author(s).
Conflict of interest statement
Dr. Novak is advisor/independent contractor for Dysimmune Diseases Foundation. He received royalties from Oxford University Press. Dr. Novak owns or owned stocks or stock options of Pfizer, Moderna, Editas Medicine and Novavax. The remaining authors have no competing interests as defined by Nature Research, or other interests that might be perceived to influence the results and/or discussion reported in this paper.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
