

Prognosis prediction and risk stratification of transarterial chemoembolization or intraarterial chemotherapy for unresectable hepatocellular carcinoma based on machine learning
- PMID: 38291256
- PMCID: PMC11255051
- DOI: 10.1007/s00330-024-10581-2
Prognosis prediction and risk stratification of transarterial chemoembolization or intraarterial chemotherapy for unresectable hepatocellular carcinoma based on machine learning
Abstract
Objective: To develop and validate a risk scoring scale model (RSSM) for stratifying prognostic risk after intra-arterial therapies (IATs) for hepatocellular carcinoma (HCC).
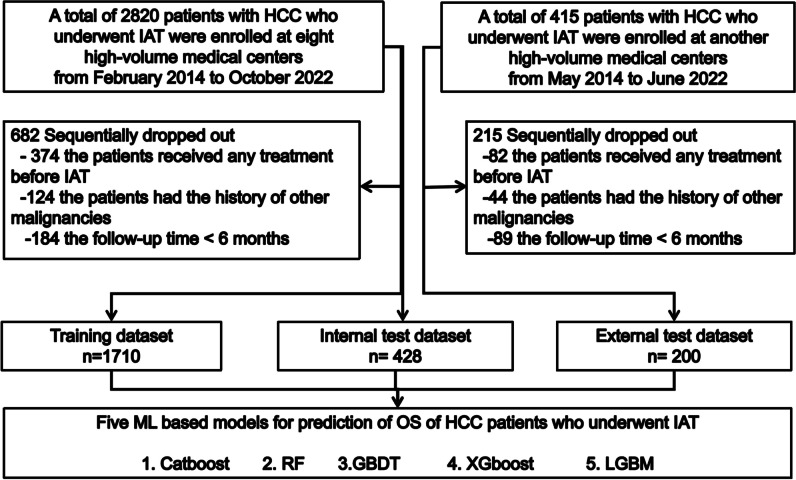
Methods: Between February 2014 and October 2022, 2338 patients with HCC who underwent initial IATs were consecutively enrolled. These patients were divided into training datasets (TD, n = 1700), internal validation datasets (ITD, n = 428), and external validation datasets (ETD, n = 200). Five-years death was used to predict outcome. Thirty-four clinical information were input and five supervised machine learning (ML) algorithms, including eXtreme Gradient Boosting (XGBoost), Categorical Gradient Boosting (CatBoost), Gradient Boosting Decision Tree (GBDT), Light Gradient Boosting Machine (LGBT), and Random Forest (RF), were compared using the areas under the receiver operating characteristic (AUC) with DeLong test. The variables with top important ML scores were used to build the RSSM by stepwise Cox regression.
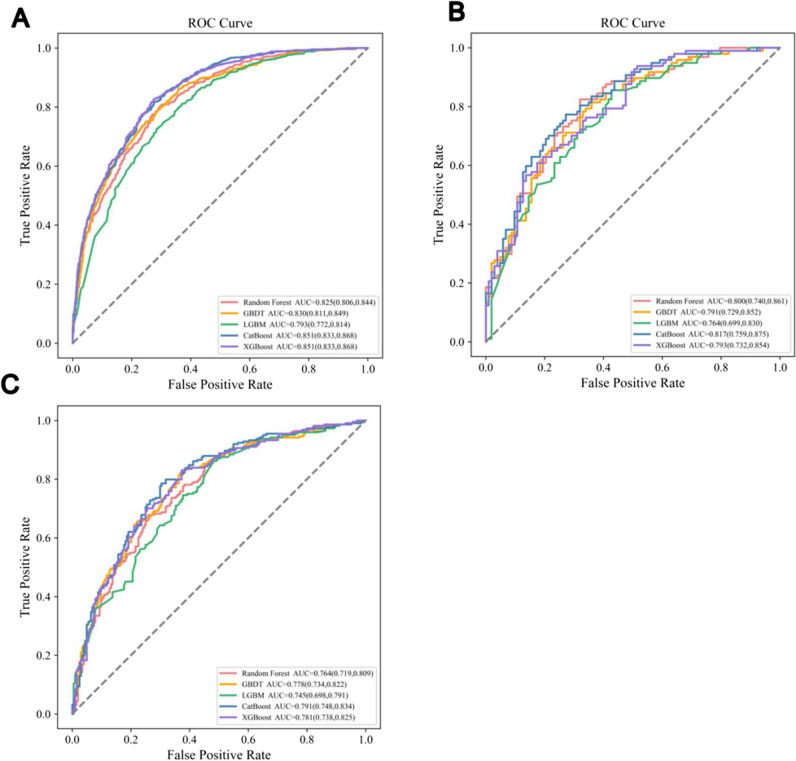
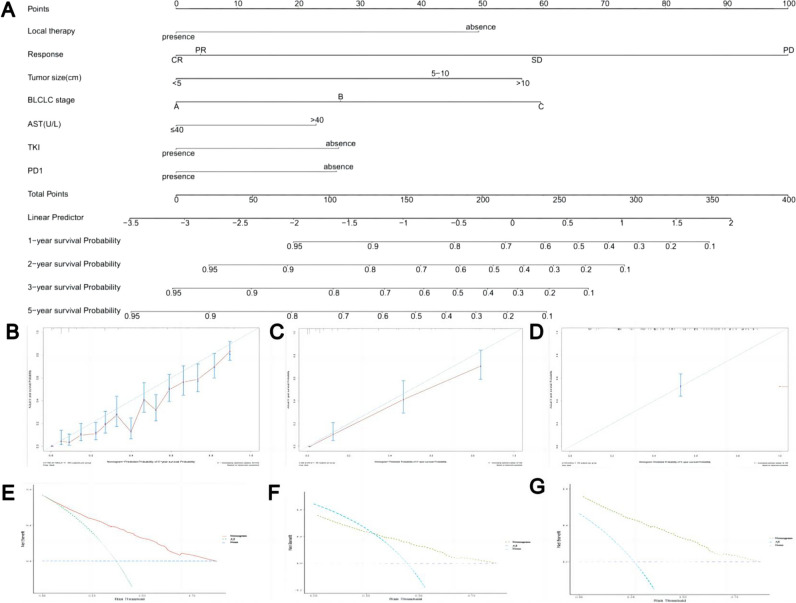
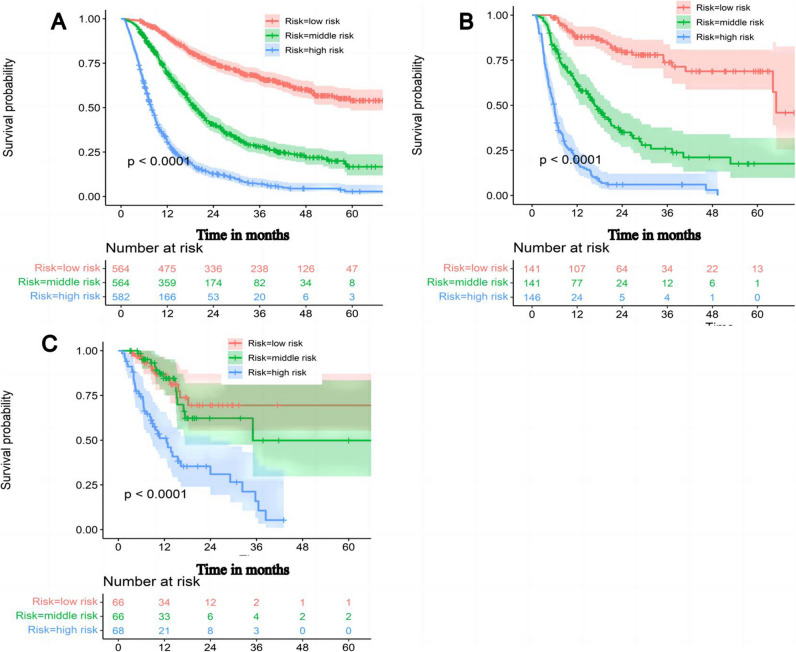
Results: The CatBoost model achieved the best discrimination when 12 top variables were input, with the AUC of 0.851 (95% confidence intervals (CI), 0.833-0.868) for TD, 0.817 (95%CI, 0.759-0.857) for ITD, and 0.791 (95%CI, 0.748-0.834) for ETD. The RSSM was developed based on the immune checkpoint inhibitors (ICI) (hazard ratios (HR), 0.678; 95%CI 0.549, 0.837), tyrosine kinase inhibitors (TKI) (HR, 0.702; 95%CI 0.605, 0.814), local therapy (HR, 0.104; 95%CI 0.014, 0.747), response to the first IAT (HR, 4.221; 95%CI 2.229, 7.994), tumor size (HR, 1.054; 95%CI 1.038, 1.070), and BCLC grade (HR, 2.375; 95%CI 1.950, 2.894). Kaplan-Meier analysis confirmed the role of RSSM in risk stratification (p < 0.001).
Conclusions: The RSSM can stratify accurately prognostic risk for HCC patients received IAT. On the basis, an online calculator permits easy implementation of this model.
Clinical relevance statement: The risk scoring scale model could be easily implemented for physicians to stratify risk and predict prognosis quickly and accurately, thereby serving as a more favorable tool to strengthen individualized intra-arterial therapies and management in patients with unresectable hepatocellular carcinoma.
Key points: • The Categorical Gradient Boosting (CatBoost) algorithm achieved the optimal and robust predictive ability (AUC, 0.851 (95%CI, 0.833-0.868) in training datasets, 0.817 (95%CI, 0.759-0.857) in internal validation datasets, and 0.791 (95%CI, 0.748-0.834) in external validation datasets) for prediction of 5-years death of hepatocellular carcinoma (HCC) after intra-arterial therapies (IATs) among five machine learning models. • We used the SHapley Additive exPlanations algorithms to explain the CatBoost model so as to resolve the black boxes of machine learning principles. • A simpler restricted variable, risk scoring scale model (RSSM), derived by stepwise Cox regression for risk stratification after intra-arterial therapies for hepatocellular carcinoma, provides the potential forewarning to adopt combination strategies for high-risk patients.
Keywords: Hepatocellular carcinoma; Intra-arterial therapies; Machine learning; Risk scoring scale model; Risk stratification.
© 2024. The Author(s).
Conflict of interest statement
The authors of this manuscript declare no relationships with any companies, whose products or services may be related to the subject matter of the article.
Figures
Similar articles
-
Machine learning-based decision support model for selecting intra-arterial therapies for unresectable hepatocellular carcinoma: A national real-world evidence-based study.Br J Cancer. 2024 Sep;131(5):832-842. doi: 10.1038/s41416-024-02784-7. Epub 2024 Jul 6. Br J Cancer. 2024. PMID: 38971951 Free PMC article.
-
Machine learning-based model for predicting tumor recurrence after interventional therapy in HBV-related hepatocellular carcinoma patients with low preoperative platelet-albumin-bilirubin score.Front Immunol. 2024 May 28;15:1409443. doi: 10.3389/fimmu.2024.1409443. eCollection 2024. Front Immunol. 2024. PMID: 38863693 Free PMC article.
-
Computed tomography radiomic features and clinical factors predicting the response to first transarterial chemoembolization in intermediate-stage hepatocellular carcinoma.Hepatobiliary Pancreat Dis Int. 2024 Aug;23(4):361-369. doi: 10.1016/j.hbpd.2023.06.011. Epub 2023 Jul 5. Hepatobiliary Pancreat Dis Int. 2024. PMID: 37429785
-
Interpretable machine learning model to predict surgical difficulty in laparoscopic resection for rectal cancer.Front Oncol. 2024 Feb 6;14:1337219. doi: 10.3389/fonc.2024.1337219. eCollection 2024. Front Oncol. 2024. PMID: 38380369 Free PMC article. Review.
-
Precision Strike Strategy for Liver Diseases Trilogy with Xiao-Chai-Hu Decoction: A Meta-Analysis with Machine Learning.Phytomedicine. 2025 Jul;142:156796. doi: 10.1016/j.phymed.2025.156796. Epub 2025 Apr 23. Phytomedicine. 2025. PMID: 40347886
Cited by
-
Applications of artificial intelligence in interventional oncology: An up-to-date review of the literature.Jpn J Radiol. 2025 Feb;43(2):164-176. doi: 10.1007/s11604-024-01668-3. Epub 2024 Oct 2. Jpn J Radiol. 2025. PMID: 39356439 Free PMC article. Review.
-
Integrating Bulk and Single-Cell RNA Sequencing Data Reveals the Prognostic Significance of HOXC9-Related Immune Gene Signatures in Hepatocellular Carcinoma.Onco Targets Ther. 2025 Mar 29;18:453-465. doi: 10.2147/OTT.S509625. eCollection 2025. Onco Targets Ther. 2025. PMID: 40177614 Free PMC article.
-
Machine learning-based decision support model for selecting intra-arterial therapies for unresectable hepatocellular carcinoma: A national real-world evidence-based study.Br J Cancer. 2024 Sep;131(5):832-842. doi: 10.1038/s41416-024-02784-7. Epub 2024 Jul 6. Br J Cancer. 2024. PMID: 38971951 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
