

Surgical Versus Dilational Tracheostomy in Patients with Severe Stroke: A SETPOINT2 Post hoc Analysis
- PMID: 38291277
- PMCID: PMC11335838
- DOI: 10.1007/s12028-023-01933-9
Surgical Versus Dilational Tracheostomy in Patients with Severe Stroke: A SETPOINT2 Post hoc Analysis
Abstract
Background: Tracheostomy in mechanically ventilated patients with severe stroke can be performed surgically or dilationally. Prospective data comparing both methods in patients with stroke are scarce. The randomized Stroke-Related Early Tracheostomy vs Prolonged Orotracheal Intubation in Neurocritical Care Trial2 (SETPOINT2) assigned 382 mechanically ventilated patients with stroke to early tracheostomy versus extubation or standard tracheostomy. Surgical tracheostomy (ST) was performed in 41 of 307 SETPOINT2 patients, and the majority received dilational tracheostomy (DT). We aimed to compare ST and DT in these patients with patients.
Methods: All SETPOINT2 patients with ST were compared with a control group of patients with stroke undergoing DT (1:2), selected by propensity score matching that included the factors stroke type, SETPOINT2 randomization group, Stroke Early Tracheostomy score, patient age, and premorbid functional status. Successful decannulation was the primary outcome, and secondary outcome parameters included functional outcome at 6 months and adverse events attributable to tracheostomy. Potential predictors of decannulation were evaluated by regression analysis.
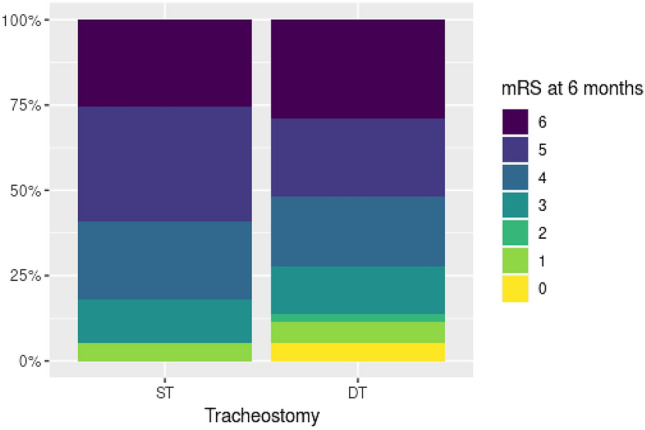
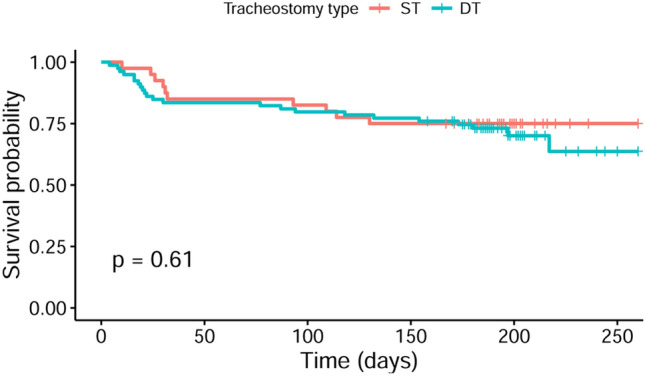
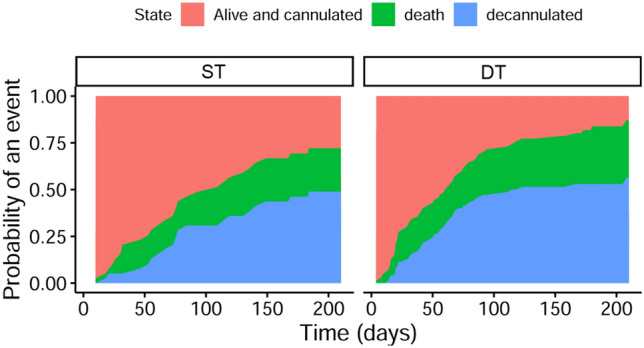
Results: Baseline characteristics were comparable in the two groups of patients with stroke undergoing ST (n = 41) and matched patients with stroke undergoing DT (n = 82). Tracheostomy was performed significantly later in the ST group than in the DT group (median 9 [interquartile range {IQR} 5-12] vs. 9 [IQR 4-11] days after intubation, p = 0.025). Patients with ST were mechanically ventilated longer (median 19 [IQR 17-24] vs.14 [IQR 11-19] days, p = 0.008) and stayed in the intensive care unit longer (median 23 [IQR 16-27] vs. 17 [IQR 13-24] days, p = 0.047), compared with patients with DT. The intrahospital infection rate was significantly higher in the ST group compared to the DT group (14.6% vs. 1.2%, p = 0.002). At 6 months, decannulation rates (56% vs. 61%), functional outcomes, and mortality were not different. However, decannulation was performed later in the ST group compared to the DT group (median 81 [IQR 66-149] vs. 58 [IQR 32-77] days, p = 0.004). Higher baseline Stroke Early Tracheostomy score negatively predicted decannulation.
Conclusions: In ventilated patients with severe stroke in need of tracheostomy, surgical and dilational methods are associated with comparable decannulation rate and functional outcome at 6 months. However, ST was associated with longer time to decannulation and higher rates of early infections, supporting the dilational approach to tracheostomy in ventilated patients with stroke.
Keywords: Decannulation; Intracerebral hemorrhage; Ischemic stroke; Stroke; Subarachnoid hemorrhage; Tracheostomy.
© 2024. The Author(s).
Conflict of interest statement
HS, JM, CK, WDN, DBS, and JB particpated in the SETPOINT2 trial, supported by the Patient-Centered Outcomes Research Institute, award reference CER 1602–34137.
Figures
Similar articles
-
Early tracheostomy in ventilated stroke patients: Study protocol of the international multicentre randomized trial SETPOINT2 (Stroke-related Early Tracheostomy vs. Prolonged Orotracheal Intubation in Neurocritical care Trial 2).Int J Stroke. 2016 Apr;11(3):368-79. doi: 10.1177/1747493015616638. Epub 2016 Jan 5. Int J Stroke. 2016. PMID: 26763913 Clinical Trial.
-
Benefits of early tracheostomy in ventilated stroke patients? Current evidence and study protocol of the randomized pilot trial SETPOINT (Stroke-related Early Tracheostomy vs. Prolonged Orotracheal Intubation in Neurocritical care Trial).Int J Stroke. 2012 Feb;7(2):173-82. doi: 10.1111/j.1747-4949.2011.00703.x. Int J Stroke. 2012. PMID: 22264372 Clinical Trial.
-
Decannulation and Functional Outcome After Tracheostomy in Patients with Severe Stroke (DECAST): A Prospective Observational Study.Neurocrit Care. 2017 Aug;27(1):26-34. doi: 10.1007/s12028-017-0390-y. Neurocrit Care. 2017. PMID: 28324263
-
Tracheostomy timing and outcome in critically ill patients with stroke: a meta-analysis and meta-regression.Crit Care. 2023 Apr 1;27(1):132. doi: 10.1186/s13054-023-04417-6. Crit Care. 2023. PMID: 37005666 Free PMC article.
-
Tracheostomy: from insertion to decannulation.Can J Surg. 2009 Oct;52(5):427-33. Can J Surg. 2009. PMID: 19865580 Free PMC article. Review.
Cited by
-
Tracheostomy Practice in the Italian Intensive Care Units: A Point-Prevalence Survey.Medicina (Kaunas). 2025 Jan 7;61(1):87. doi: 10.3390/medicina61010087. Medicina (Kaunas). 2025. PMID: 39859070 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
