

Immunogenicity and reactogenicity of modified vaccinia Ankara pre-exposure vaccination against mpox according to previous smallpox vaccine exposure and HIV infection: prospective cohort study
- PMID: 38292040
- PMCID: PMC10825638
- DOI: 10.1016/j.eclinm.2023.102420
Immunogenicity and reactogenicity of modified vaccinia Ankara pre-exposure vaccination against mpox according to previous smallpox vaccine exposure and HIV infection: prospective cohort study
Abstract
Background: Pre-exposure vaccination with MVA-BN has been widely used against mpox to contain the 2022 outbreak. Many countries have defined prioritized strategies, administering a single dose to those historically vaccinated for smallpox, to achieve quickly adequate coverage in front of low supplies. Using epidemiological models, real-life effectiveness was estimated at approximately 36%-86%, but no clinical trials were performed. Few data on MVA-BN immunogenicity are currently available, and there are no established correlates of protection. Immunological response in PLWH in the context of the 2022 outbreak was also poorly described.
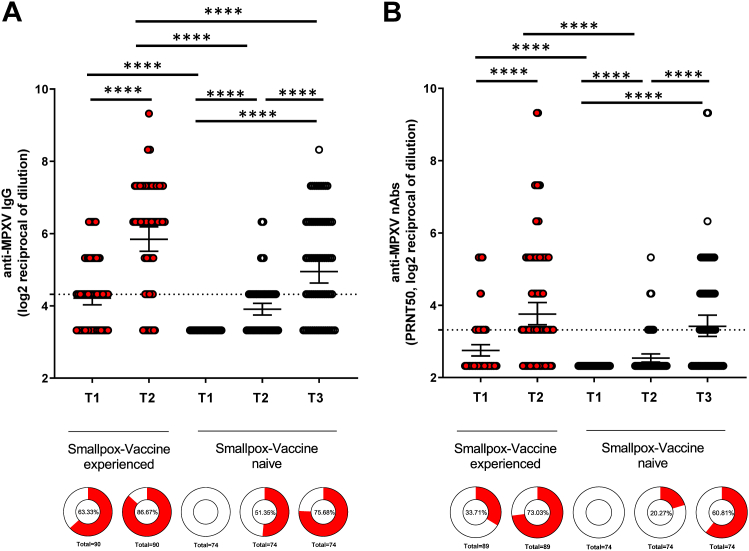
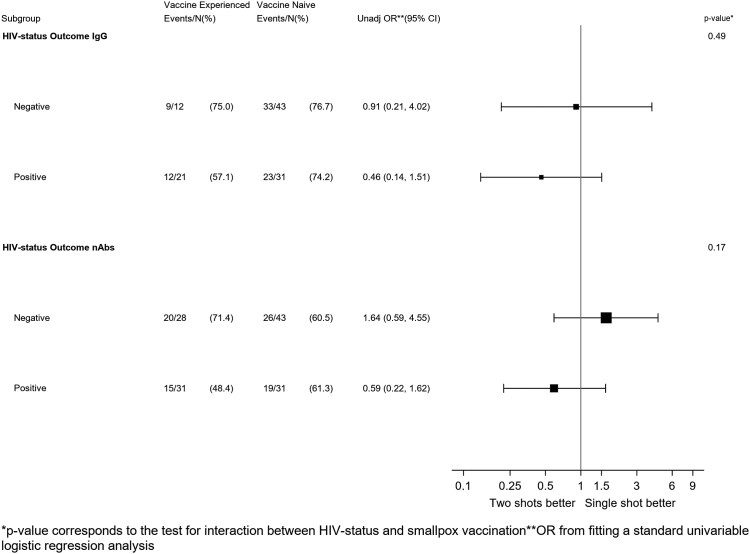
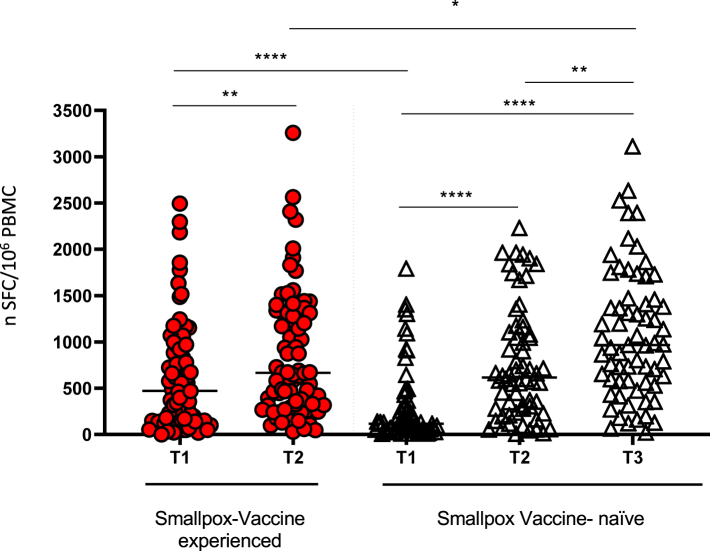
Methods: Blood samples were collected from participants eligible for pre-exposure MVA-BN vaccination before (T1) receiving a full course of vaccine (single-dose for vaccine-experienced or smallpox-primed and two-dose for smallpox vaccine-naïve or smallpox non-primed) and one month after the last dose (T2 and T3, respectively). MPXV-specific IgGs were measured by in-house immunofluorescence assay, using 1:20 as screening dilution, MPXV-specific nAbs by 50% plaque reduction neutralization test (PRNT50, starting dilution 1:10), and IFN-γ-producing specific T cells to MVA-BN vaccine, by ELISpot assay. Paired or unpaired t-test and Wilcoxon or Mann-Whitney test were used to analyse IgG and nAbs, and T-cell response, as appropriate. The probability of IgG and nAb response in vaccine-experienced vs. vaccine-naïve was estimated in participants not reactive at T1. The McNemar test was used to evaluate vaccination's effect on humoral response both overall and by smallpox vaccination history. In participants who were not reactive at T1, the proportion of becoming responders one month after full-cycle completion by exposure groups was compared by logistic regression and then analysed by HIV status strata (interaction test). The response was also examined in continuous, and the Average Treatment Effect (ATE) of the difference from baseline to schedule completion according to previous smallpox vaccination was estimated after weighting for HIV using a linear regression model. Self-reports of adverse effects following immunization (AEFIs) were prospectively collected after the first MVA-BN dose (T1). Systemic (S-AEFIs: fatigue, myalgia, headache, GI effects, chills) and local (L-AEFIs: redness, swelling, pain) AEFIs were graded as absent (grade 0), mild (1), moderate (2), or severe (3). The maximum level of severity for S-AEFIs and L-AEFIs ever experienced over the 30 days post-dose by vaccination exposure groups were analysed using a univariable multinomial logistic regression model and after adjusting for HIV status; for each of the symptoms, we also compared the mean duration by exposure group using an unpaired t-test.
Findings: Among the 164 participants included, 90 (54.8%) were smallpox vaccine-experienced. Median age was 49 years (IQR 41-55). Among the 76 (46%) PLWH, 76% had a CD4 count >500 cells/μL. There was evidence that both the IgG and nAbs titers increased after administration of the MVA-BN vaccine. However, there was no evidence for a difference in the potential mean change in humoral response from baseline to the completion of a full cycle when comparing primed vs. non-primed participants. Similarly, there was no evidence for a difference in the seroconversion rate after full cycle vaccination in the subset of participants not reactive for nAbs at T1 (p = 1.00 by Fisher's exact test). In this same analysis and for the nAbs outcome, there was some evidence of negative effect modification by HIV (interaction p-value = 0.17) as primed people living with HIV (PLWH) showed a lower probability of seroconversion vs. non-primed, and the opposite was seen in PLWoH. When evaluating the response in continuous, we observed an increase in T-cell response after MVA-BN vaccination in both primed and non-primed. There was evidence for a larger increase when using the 2-dose vs. one-dose strategy with a mean difference of -2.01 log2 (p ≤ 0.0001), after controlling for HIV. No evidence for a difference in the risk of developing any AEFIs of any grade were observed by exposure group, except for the lower risk of grade 2 (moderate) fatigue, induration and local pain which was lower in primed vs. non-primed [OR 0.26 (0.08-0.92), p = 0.037; OR 0.30 (0.10-0.88), p = 0.029 and OR 0.19 (0.05-0.73), p = 0.015, respectively]. No evidence for a difference in symptom duration was also detected between the groups.
Interpretation: The evaluation of the humoral and cellular response one month after the completion of the vaccination cycle suggested that MVA-BN is immunogenic and that the administration of a two-dose schedule is preferable regardless of the previous smallpox vaccination history, especially in PLWH, to maximize nAbs response. MVA-BN was safe as well tolerated, with grade 2 reactogenicity higher after the first administration in vaccine-naïve than in vaccine-experienced individuals, but with no evidence for a difference in the duration of these adverse effects. Further studies are needed to evaluate the long-term duration of immunity and to establish specific correlates of protection.
Funding: The study was supported by the National Institute for Infectious Disease Lazzaro Spallanzani IRCCS "Advanced grant 5 × 1000, 2021" and by the Italian Ministry of Health "Ricerca Corrente Linea 2".
Keywords: Cellular response; HIV; Humoral response; MVA-BN; MVA-BN immunogenicity; Orthopox; PLWH; Reactogenicity; Vaccination; Vaccine; mpox.
© 2023 The Author(s).
Conflict of interest statement
The authors declare that no conflicting financial interests or other competing relationships exist.
Figures
References
-
- Centers and Disease Control and Prevention . 2022. Monkeypox outbreak global map. 2023. Data as of October 25th 2023 at 5:30 pm EDT.
LinkOut - more resources
Full Text Sources
Research Materials
