

New trends in diagnosis and management of gallbladder carcinoma
- PMID: 38292841
- PMCID: PMC10824116
- DOI: 10.4251/wjgo.v16.i1.13
New trends in diagnosis and management of gallbladder carcinoma
Abstract
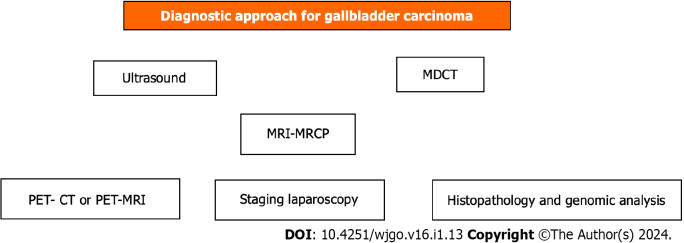
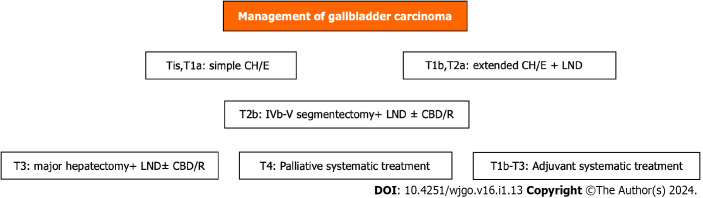
Gallbladder (GB) carcinoma, although relatively rare, is the most common biliary tree cholangiocarcinoma with aggressiveness and poor prognosis. It is closely associated with cholelithiasis and long-standing large (> 3 cm) gallstones in up to 90% of cases. The other main predisposing factors for GB carcinoma include molecular factors such as mutated genes, GB wall calcification (porcelain) or mainly mucosal microcalcifications, and GB polyps ≥ 1 cm in size. Diagnosis is made by ultrasound, computed tomography (CT), and, more precisely, magnetic resonance imaging (MRI). Preoperative staging is of great importance in decision-making regarding therapeutic management. Preoperative staging is based on MRI findings, the leading technique for liver metastasis imaging, enhanced three-phase CT angiography, or magnetic resonance angiography for major vessel assessment. It is also necessary to use positron emission tomography (PET)-CT or 18F-FDG PET-MRI to more accurately detect metastases and any other occult deposits with active metabolic uptake. Staging laparoscopy may detect dissemination not otherwise found in 20%-28.6% of cases. Multimodality treatment is needed, including surgical resection, targeted therapy by biological agents according to molecular testing gene mapping, chemotherapy, radiation therapy, and immunotherapy. It is of great importance to understand the updated guidelines and current treatment options. The extent of surgical intervention depends on the disease stage, ranging from simple cholecystectomy (T1a) to extended resections and including extended cholecystectomy (T1b), with wide lymph node resection in every case or IV-V segmentectomy (T2), hepatic trisegmentectomy or major hepatectomy accompanied by hepaticojejunostomy Roux-Y, and adjacent organ resection if necessary (T3). Laparoscopic or robotic surgery shows fewer postoperative complications and equivalent oncological outcomes when compared to open surgery, but much attention must be paid to avoiding injuries. In addition to surgery, novel targeted treatment along with immunotherapy and recent improvements in radiotherapy and chemotherapy (neoadjuvant-adjuvant capecitabine, cisplatin, gemcitabine) have yielded promising results even in inoperable cases calling for palliation (T4). Thus, individualized treatment must be applied.
Keywords: Biliary tract neoplasms; Biliary tree diseases; Extrahepatic cholangiocarcinoma; Gallbladder carcinoma; Gallbladder diseases; Gastrointestinal malignancies.
©The Author(s) 2024. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: There is no conflict of interest associated with the senior author or any of the other coauthors who contributed their efforts in this manuscript.
Figures
References
-
- Vuthaluru S, Sharma P, Chowdhury S, Are C. Global epidemiological trends and variations in the burden of gallbladder cancer. J Surg Oncol. 2023;128:980–988. - PubMed
-
- Balakrishnan A, Barmpounakis P, Demiris N, Jah A, Spiers HVM, Talukder S, Martin JL, Gibbs P, Harper SJF, Huguet EL, Kosmoliaptsis V, Liau SS, Praseedom RK, Basu B, de Aretxabala X, Lendoire J, Maithel S, Branes A, Andersson B, Serrablo A, Adsay V OMEGA Study Investigators. Surgical outcomes of gallbladder cancer: the OMEGA retrospective, multicentre, international cohort study. EClinicalMedicine. 2023;59:101951. - PMC - PubMed
-
- Laurenzi A, Brandi G, Greco F, Prosperi E, Palloni A, Serenari M, Frega G, Ravaioli M, Rizzo A, Cescon M. Can repeated surgical resection offer a chance of cure for recurrent cholangiocarcinoma? Langenbecks Arch Surg. 2023;408:102. - PubMed
-
- Kim D, Konyn P, Cholankeril G, Bonham CA, Ahmed A. Trends in the Mortality of Biliary Tract Cancers Based on Their Anatomical Site in the United States From 2009 to 2018. Am J Gastroenterol. 2021;116:1053–1062. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
