

An early warning model to predict acute kidney injury in sepsis patients with prior hypertension
- PMID: 38293505
- PMCID: PMC10827515
- DOI: 10.1016/j.heliyon.2024.e24227
An early warning model to predict acute kidney injury in sepsis patients with prior hypertension
Abstract
Background: In the context of sepsis patients, hypertension has a significant impact on the likelihood of developing sepsis-associated acute kidney injury (S-AKI), leading to a considerable burden. Moreover, sepsis is responsible for over 50 % of cases of acute kidney injuries (AKI) and is linked to an increased likelihood of death during hospitalization. The objective of this research is to develop a dependable and strong nomogram framework, utilizing the variables accessible within the first 24 h of admission, for the anticipation of S-AKI in sepsis patients who have hypertension.
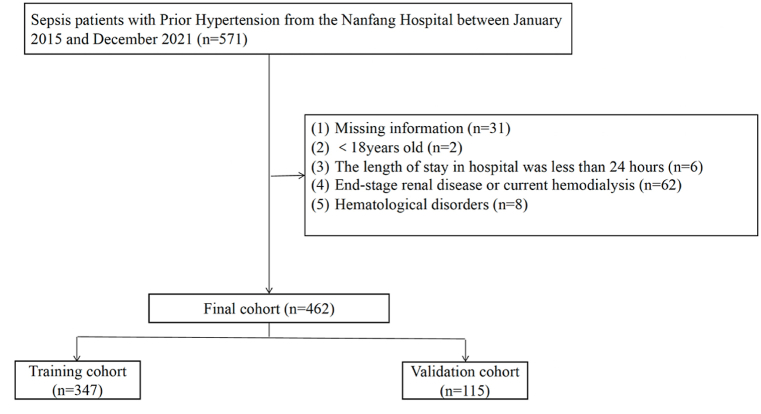
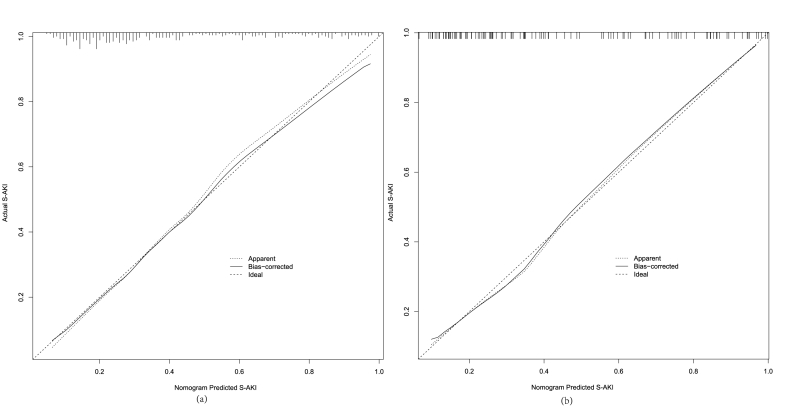
Methods: In this study that looked back, a total of 462 patients with sepsis and high blood pressure were identified from Nanfang Hospital. These patients were then split into a training set (consisting of 347 patients) and a validation set (consisting of 115 patients). A multivariate logistic regression analysis and a univariate logistic regression analysis were performed to identify the factors that independently predict S-AKI. Based on these independent predictors, the model was constructed. To evaluate the efficacy of the designed nomogram, several analyses were conducted, including calibration curves, receiver operating characteristics curves, and decision curve analysis.
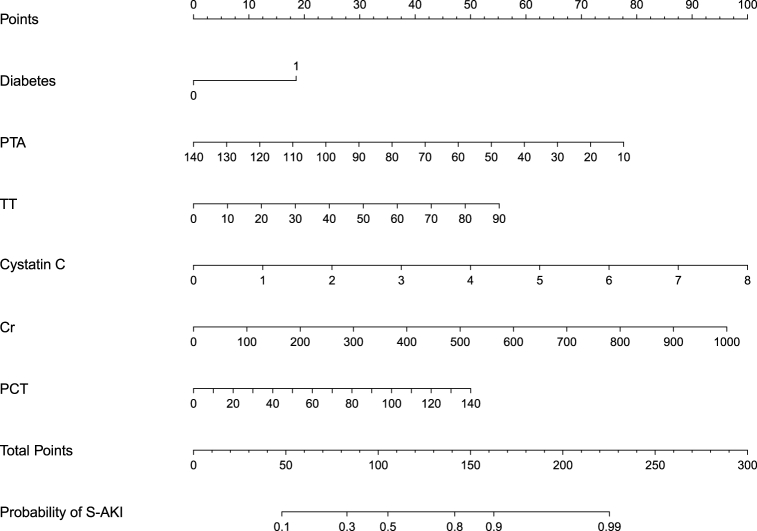
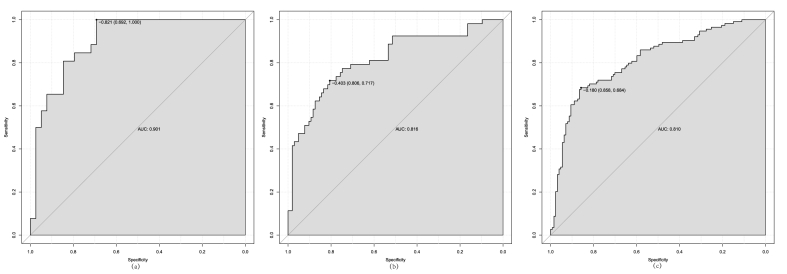
Results: The findings of this research indicated that diabetes, prothrombin time activity (PTA), thrombin time (TT), cystatin C, creatinine (Cr), and procalcitonin (PCT) were autonomous prognosticators for S-AKI in sepsis individuals with hypertension. The nomogram model, built using these predictors, demonstrated satisfactory discrimination in both the training (AUC = 0.823) and validation (AUC = 0.929) groups. The S-AKI nomogram demonstrated superior predictive ability in assessing S-AKI within the hypertension grade I (AUC = 0.901) set, surpassing the hypertension grade II (AUC = 0.816) and III (AUC = 0.810) sets. The nomogram exhibited satisfactory calibration and clinical utility based on the calibration curve and decision curve analysis.
Conclusion: In patients with sepsis and high blood pressure, the nomogram that was created offers a dependable and strong evaluation for predicting S-AKI. This evaluation provides valuable insights to enhance individualized treatment, ultimately resulting in improved clinical outcomes.
Keywords: Acute kidney injury; Early warning; Hypertension; Nomogram; Sepsis.
© 2024 Published by Elsevier Ltd.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures


References
-
- Arshad A., Ayaz A., Rehman S., Ukrani R.D., Akbar I., Jamil B. Progression of acute kidney injury to chronic kidney disease in sepsis survivors: 1-year follow-up study. J. Intensive Care Med. 2021;36(11):1366–1370. - PubMed
-
- Wang Z., Chen Z., Zhang L., Wang X., Hao G., Zhang Z., Shao L., Tian Y., Dong Y., Zheng C., et al. Status of hypertension in China: results from the China hypertension survey, 2012-2015. Circulation. 2018;137(22):2344–2356. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
