

Clinical practice and effect of carbon dioxide on outcomes in mechanically ventilated acute brain-injured patients: a secondary analysis of the ENIO study
- PMID: 38294526
- PMCID: PMC10907416
- DOI: 10.1007/s00134-023-07305-3
Clinical practice and effect of carbon dioxide on outcomes in mechanically ventilated acute brain-injured patients: a secondary analysis of the ENIO study
Erratum in
-
Correction: Clinical practice and effect of carbon dioxide on outcomes in mechanically ventilated acute brain-injured patients: a secondary analysis of the ENIO study.Intensive Care Med. 2024 Feb;50(2):317-318. doi: 10.1007/s00134-024-07358-y. Intensive Care Med. 2024. PMID: 38393334 Free PMC article. No abstract available.
Abstract
Purpose: The use of arterial partial pressure of carbon dioxide (PaCO2) as a target intervention to manage elevated intracranial pressure (ICP) and its effect on clinical outcomes remain unclear. We aimed to describe targets for PaCO2 in acute brain injured (ABI) patients and assess the occurrence of abnormal PaCO2 values during the first week in the intensive care unit (ICU). The secondary aim was to assess the association of PaCO2 with in-hospital mortality.
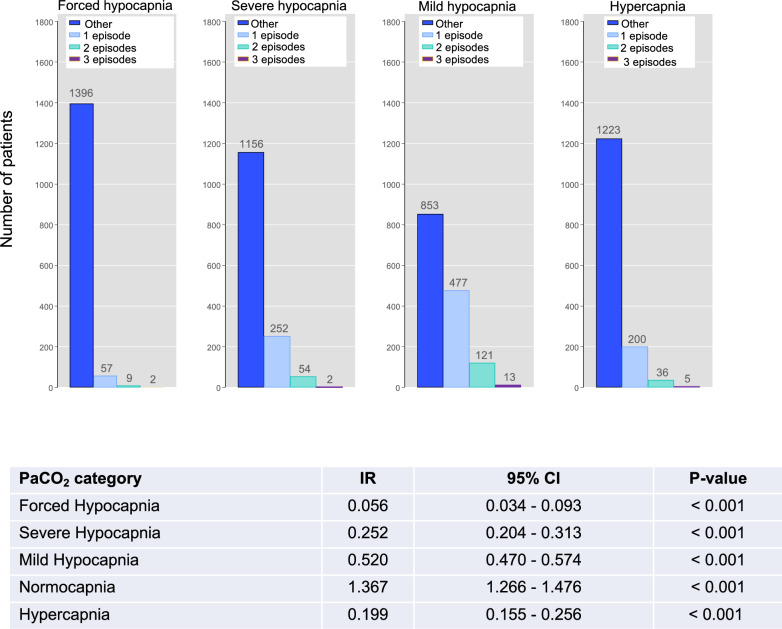
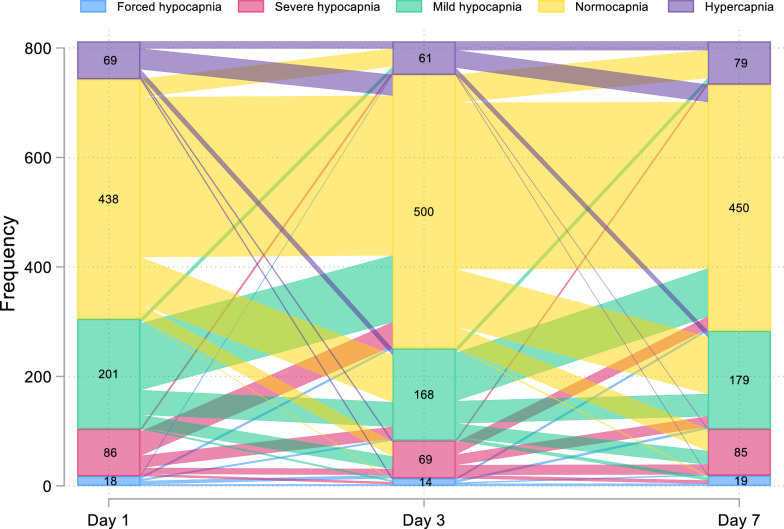
Methods: We carried out a secondary analysis of a multicenter prospective observational study involving adult invasively ventilated patients with traumatic brain injury (TBI), subarachnoid hemorrhage (SAH), intracranial hemorrhage (ICH), or ischemic stroke (IS). PaCO2 was collected on day 1, 3, and 7 from ICU admission. Normocapnia was defined as PaCO2 > 35 and to 45 mmHg; mild hypocapnia as 32-35 mmHg; severe hypocapnia as 26-31 mmHg, forced hypocapnia as < 26 mmHg, and hypercapnia as > 45 mmHg.
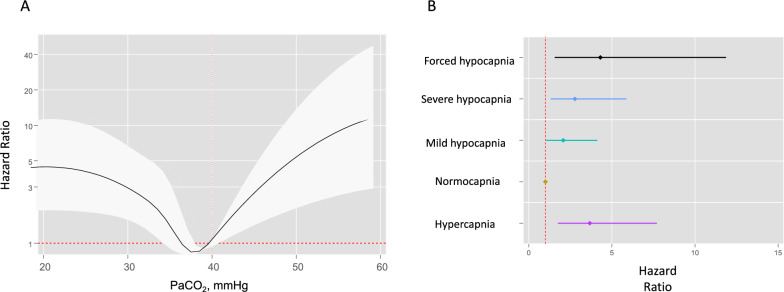
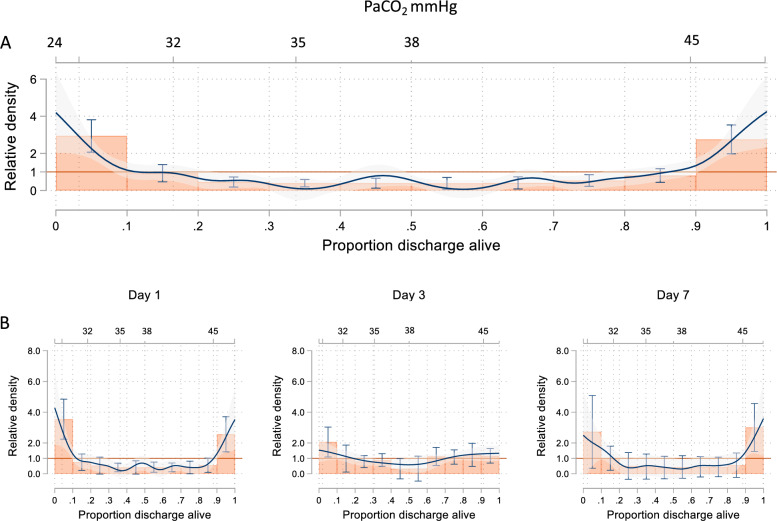
Results: 1476 patients (65.9% male, mean age 52 18 years) were included. On ICU admission, 804 (54.5%) patients were normocapnic (incidence 1.37 episodes per person/day during ICU stay), and 125 (8.5%) and 334 (22.6%) were mild or severe hypocapnic (0.52 and 0.25 episodes/day). Forced hypocapnia and hypercapnia were used in 40 (2.7%) and 173 (11.7%) patients. PaCO2 had a U-shape relationship with in-hospital mortality with only severe hypocapnia and hypercapnia being associated with increased probability of in-hospital mortality (omnibus p value = 0.0009). Important differences were observed across different subgroups of ABI patients.
Conclusions: Normocapnia and mild hypocapnia are common in ABI patients and do not affect patients' outcome. Extreme derangements of PaCO2 values were significantly associated with increased in-hospital mortality.
Keywords: Brain injury; Carbon dioxide; Critical care; Hyperventilation; ICH; Intensive care; Invasive ventilation; PaCO2; SAH; Stroke; TBI.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that the article content was composed in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Hoiland RL, Fisher JA, Ainslie PN (2019) Regulation of the cerebral circulation by arterial carbon dioxide. In: Comprehensive Physiology. Wiley, pp 1101–1154 - PubMed
-
- Chesnut R, Aguilera S, Buki A, et al. A management algorithm for adult patients with both brain oxygen and intracranial pressure monitoring: the Seattle International Severe Traumatic Brain Injury Consensus Conference (SIBICC) Intensive Care Med. 2020;46:919–929. doi: 10.1007/s00134-019-05900-x. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
