

Relationship Between Lipoprotein(a), Renal Function Indicators, and Chronic Kidney Disease: Evidence From a Large Prospective Cohort Study
- PMID: 38294877
- PMCID: PMC10867749
- DOI: 10.2196/50415
Relationship Between Lipoprotein(a), Renal Function Indicators, and Chronic Kidney Disease: Evidence From a Large Prospective Cohort Study
Abstract
Background: Chronic kidney disease (CKD) poses a significant global public health challenge. While lipoprotein(a) (Lp[a]) has been established as a significant factor in cardiovascular disease, its connection to CKD risk remains a topic of debate. Existing evidence indicates diverse risks of kidney disease among individuals with various renal function indicators, even when within the normal range.
Objective: This study aims to investigate the joint associations between different renal function indicators and Lp(a) regarding the risks of incident CKD in the general population.
Methods: The analysis involved a cohort of 329,415 participants without prior CKD who were enrolled in the UK Biobank between 2006 and 2010. The participants, with an average age of 56 (SD 8.1) years, included 154,298/329,415 (46.84%) males. At baseline, Lp(a) levels were measured using an immunoturbidimetric assay and classified into 2 groups: low (<75 nmol/L) and high (≥75 nmol/L). To assess participants' baseline renal function, we used the baseline urine albumin-to-creatinine ratio (UACR) and estimated glomerular filtration rate (eGFR). The relationship between Lp(a), renal function indicators, and the risk of CKD was evaluated using multivariable Cox regression models. These models were adjusted for various factors, including sociodemographic variables, lifestyle factors, comorbidities, and laboratory measures.
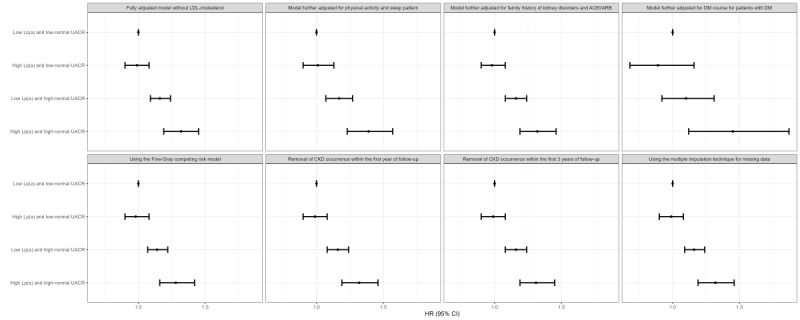
Results: A total of 6003 incident CKD events were documented over a median follow-up period of 12.5 years. The association between elevated Lp(a) levels and CKD risk did not achieve statistical significance among all participants, with a hazard ratio (HR) of 1.05 and a 95% CI ranging from 0.98 to 1.13 (P=.16). However, a notable interaction was identified between Lp(a) and UACR in relation to CKD risk (P for interaction=.04), whereas no significant interaction was observed between Lp(a) and eGFR (P for interaction=.96). When compared with the reference group with low Lp(a) and low-normal UACR (<10 mg/g), the group with high Lp(a) and low-normal UACR exhibited a nonsignificant association with CKD risk (HR 0.98, 95% CI 0.90-1.08; P=.74). By contrast, both the low Lp(a) and high-normal UACR (≥10 mg/g) group (HR 1.16, 95% CI 1.08-1.24; P<.001) and the high Lp(a) and high-normal UACR group (HR 1.32, 95% CI 1.19-1.46; P<.001) demonstrated significant associations with increased CKD risks. In individuals with high-normal UACR, elevated Lp(a) was linked to a significant increase in CKD risk, with an HR of 1.14 and a 95% CI ranging from 1.03 to 1.26 (P=.01). Subgroup analyses and sensitivity analyses consistently produced results that were largely in line with the main findings.
Conclusions: The analysis revealed a significant interaction between Lp(a) and UACR in relation to CKD risk. This implies that Lp(a) may act as a risk factor for CKD even when considering UACR. Our findings have the potential to provide valuable insights into the assessment and prevention of CKD, emphasizing the combined impact of Lp(a) and UACR from a public health perspective within the general population. This could contribute to enhancing public awareness regarding the management of Lp(a) for the prevention of CKD.
Keywords: chronic kidney disease; glomerular filtration rate; lipoprotein(a); renal function; urinary albumin-to-creatinine ratio.
©Yingxin Liu, Ruoting Wang, Shuai Li, Changfa Zhang, Gregory Y H Lip, Lehana Thabane, Guowei Li. Originally published in JMIR Public Health and Surveillance (https://publichealth.jmir.org), 31.01.2024.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures


References
-
- GBD Chronic Kidney Disease Collaboration Global, regional, and national burden of chronic kidney disease, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2020 Feb 29;395(10225):709–733. doi: 10.1016/S0140-6736(20)30045-3. https://linkinghub.elsevier.com/retrieve/pii/S0140-6736(20)30045-3 S0140-6736(20)30045-3 - DOI - PMC - PubMed
-
- Rhee CM, Kovesdy CP. Epidemiology: spotlight on CKD deaths—increasing mortality worldwide. Nat Rev Nephrol. 2015 Apr 3;11(4):199–200. doi: 10.1038/nrneph.2015.25. https://europepmc.org/abstract/MED/25734769 nrneph.2015.25 - DOI - PMC - PubMed
-
- Kidney Disease: Improving Global Outcomes (KDIGO) Glomerular Diseases Work Group KDIGO 2021 clinical practice guideline for the management of glomerular diseases. Kidney Int. 2021 Oct;100(4S):S1–S276. doi: 10.1016/j.kint.2021.05.021. https://linkinghub.elsevier.com/retrieve/pii/S0085-2538(21)00562-7 S0085-2538(21)00562-7 - DOI - PubMed
-
- Nordestgaard Børge G, Langsted Anne. Lipoprotein (a) as a cause of cardiovascular disease: insights from epidemiology, genetics, and biology. J Lipid Res. 2016 Nov;57(11):1953–1975. doi: 10.1194/jlr.R071233. https://linkinghub.elsevier.com/retrieve/pii/S0022-2275(20)34568-5 S0022-2275(20)34568-5 - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
