

Prevalence and clinical characteristics of patients with rheumatoid arthritis with interstitial lung disease using unstructured healthcare data and machine learning
- PMID: 38296310
- PMCID: PMC10836356
- DOI: 10.1136/rmdopen-2023-003353
Prevalence and clinical characteristics of patients with rheumatoid arthritis with interstitial lung disease using unstructured healthcare data and machine learning
Abstract
Objectives: Real-world data regarding rheumatoid arthritis (RA) and its association with interstitial lung disease (ILD) is still scarce. This study aimed to estimate the prevalence of RA and ILD in patients with RA (RAILD) in Spain, and to compare clinical characteristics of patients with RA with and without ILD using natural language processing (NLP) on electronic health records (EHR).
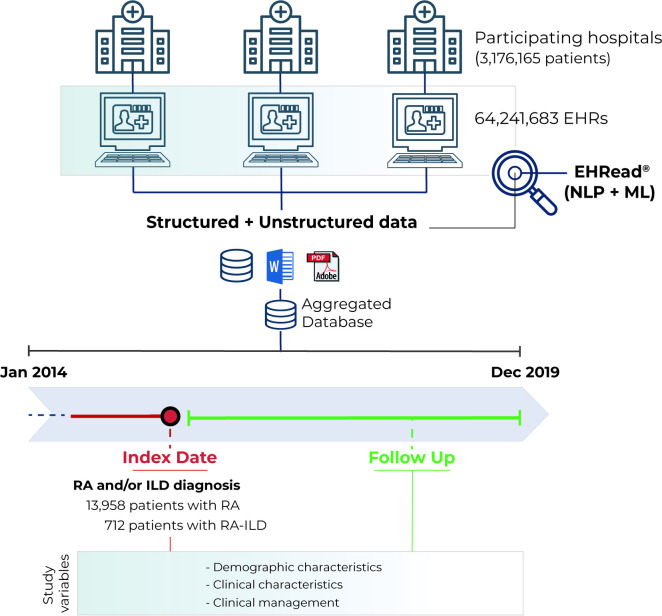
Methods: Observational case-control, retrospective and multicentre study based on the secondary use of unstructured clinical data from patients with adult RA and RAILD from nine hospitals between 2014 and 2019. NLP was used to extract unstructured clinical information from EHR and standardise it into a SNOMED-CT terminology. Prevalence of RA and RAILD were calculated, and a descriptive analysis was performed. Characteristics between patients with RAILD and RA patients without ILD (RAnonILD) were compared.
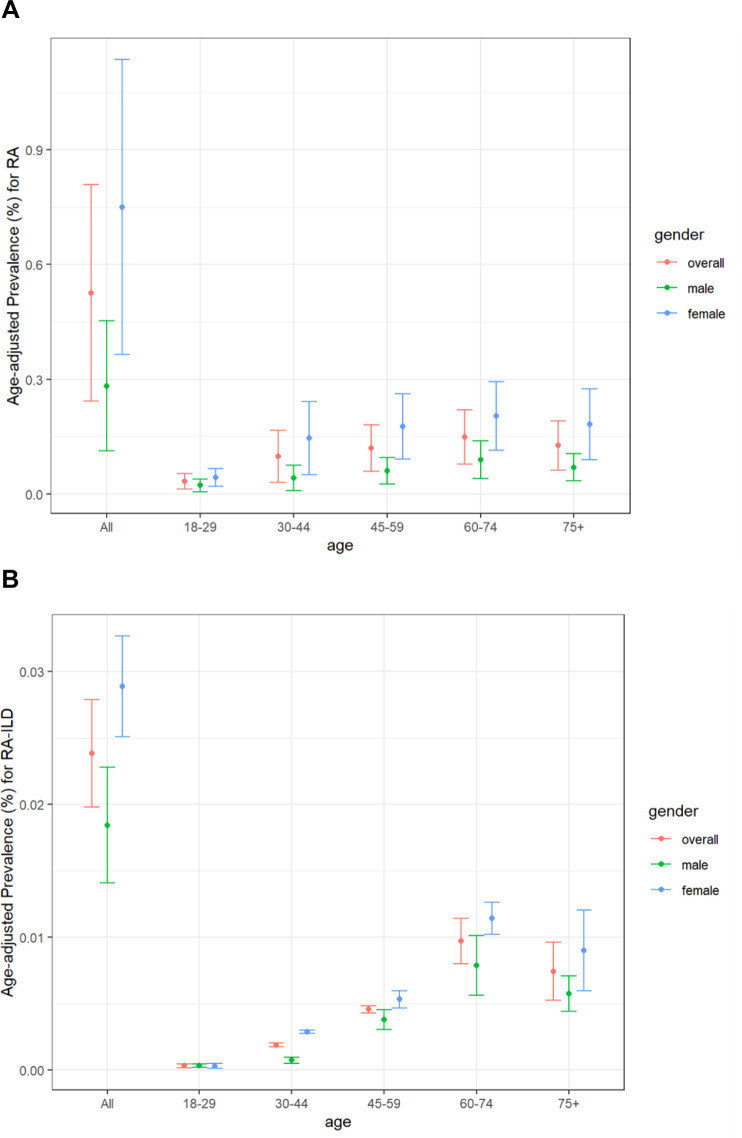
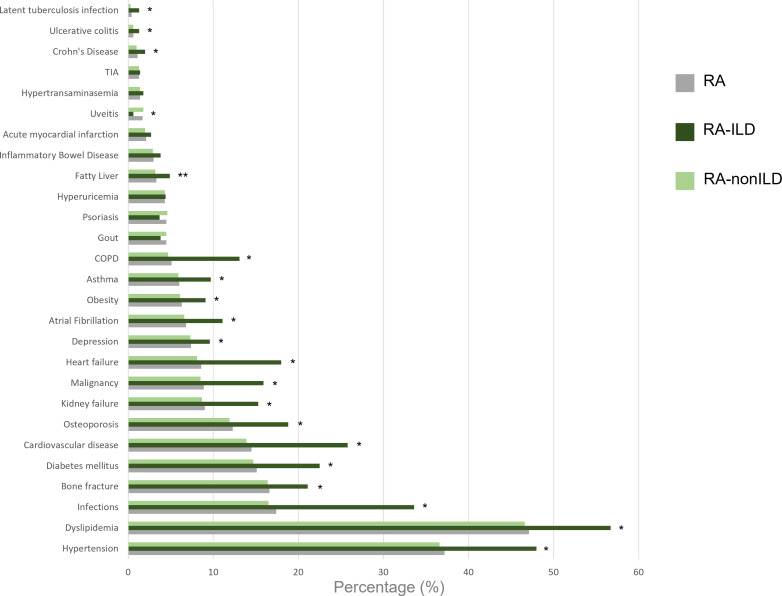
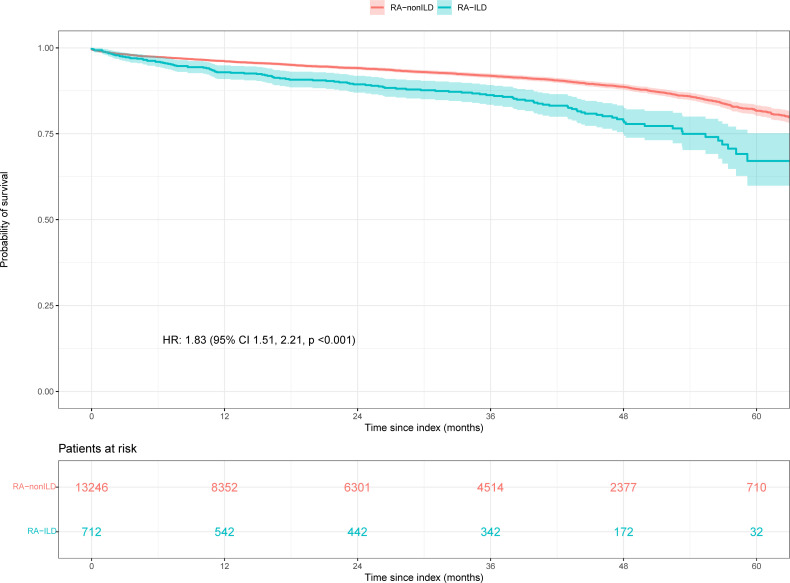
Results: From a source population of 3 176 165 patients and 64 241 683 EHRs, 13 958 patients with RA were identified. Of those, 5.1% patients additionally had ILD (RAILD). The overall age-adjusted prevalence of RA and RAILD were 0.53% and 0.02%, respectively. The most common ILD subtype was usual interstitial pneumonia (29.3%). When comparing RAILD versus RAnonILD patients, RAILD patients were older and had more comorbidities, notably concerning infections (33.6% vs 16.5%, p<0.001), malignancies (15.9% vs 8.5%, p<0.001) and cardiovascular disease (25.8% vs 13.9%, p<0.001) than RAnonILD. RAILD patients also had higher inflammatory burden reflected in more pharmacological prescriptions and higher inflammatory parameters and presented a higher in-hospital mortality with a higher risk of death (HR 2.32; 95% CI 1.59 to 2.81, p<0.001).
Conclusions: We found an estimated age-adjusted prevalence of RA and RAILD by analysing real-world data through NLP. RAILD patients were more vulnerable at the time of inclusion with higher comorbidity and inflammatory burden than RAnonILD, which correlated with higher mortality.
Keywords: Arthritis, Rheumatoid; Epidemiology; Pulmonary Fibrosis.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: JARI has received support for research grants or contracts from BMS. ET-A has received payment honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from BMS, and support for attending meetings from Boehringer Ingelheim, Nordic Pharma and Merck Sharp & Dohme. JF-M has received payment honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from BMS, Amgen, Lilly, Galápagos, Boehringer Ingelheim, Novartis and also support for attending meetings from Boehringer Ingelheim. LS-F has received payment honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Novartis, BMS, Lilly, support for attending meetings from Pfizer, Lilly and Novartis and also has participated on Data Safety Monitoring Board or Advisory Board for Novartis, Merck Sharp & Dohme and Sanofi. BS has received consulting fees from Boehringer Ingelheim, payment honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Roche and Boehriner Ingelheim, support for attending meetings from Boehringer Ingelheim, Roche and AstraZeneca. JLA has received consulting fees from AbbVie, Amgen, AstraZeneca, Biogen, Cellgene, Celltion, Fresenius-Kabi, Galápagos, Gebro, GSK, Merck Sharp & Dohme, Pfizer, Regeneron, UCB, payment honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from AbbVie, Antares, Biogen, GSK, Janssen, Merck Sharp & Dohme, Lilly, Nordic, Novartis, Sanofi, UCB and also support for attendings from AbbVie, Gebro, Janssen, Merck Sharp & Dohme, Nordic, Novartis and Pfizer. EB has received payment honoraria for educational events from Boehringer Ingelheim, support for attending meetings and/or travel from Boehringer Ingelheim and Janssen. DB currently works at Savana Research, has received grants or contracts from Novartis, payment honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Janssen and AbbVie, support for attending meetings from UCB, Novartis and AbbVie. DV works at BMS Company and own stocks as BMS employee. SLV works at BMS Company and own stocks as BMS employee. RACM works at BMS Company. The present manuscript was fully supported by Bristol-Myers Squibb.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical