

Impact of biologically effective dose on tremor decrease after stereotactic radiosurgical thalamotomy for essential tremor: a retrospective longitudinal analysis
- PMID: 38296852
- PMCID: PMC10830596
- DOI: 10.1007/s10143-024-02296-1
Impact of biologically effective dose on tremor decrease after stereotactic radiosurgical thalamotomy for essential tremor: a retrospective longitudinal analysis
Abstract
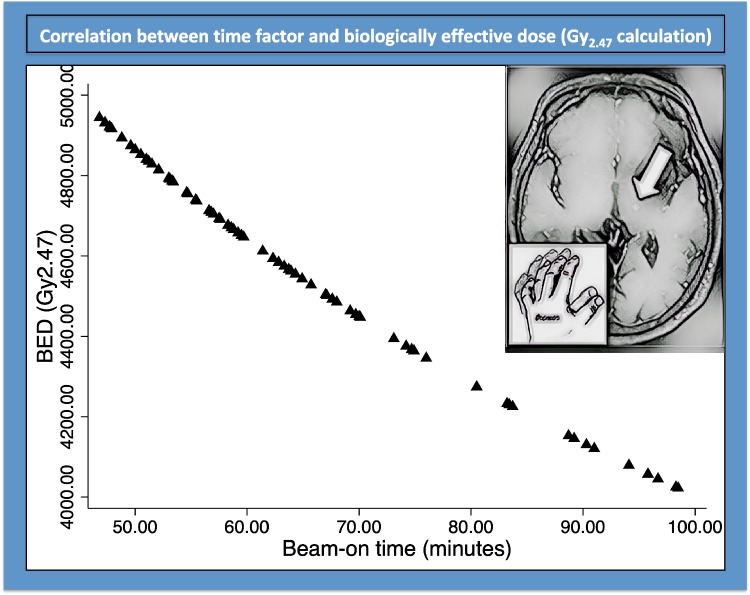
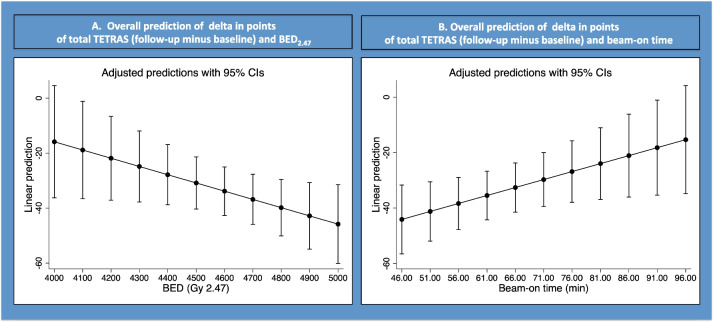
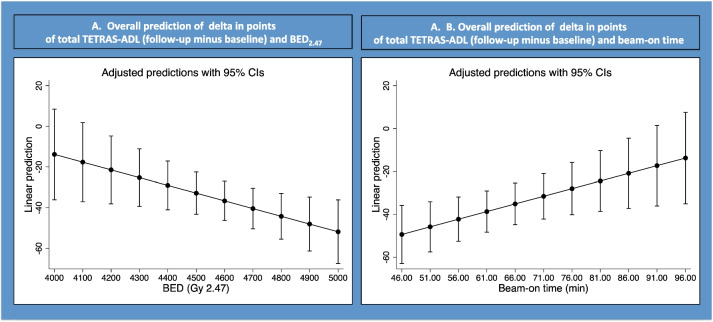
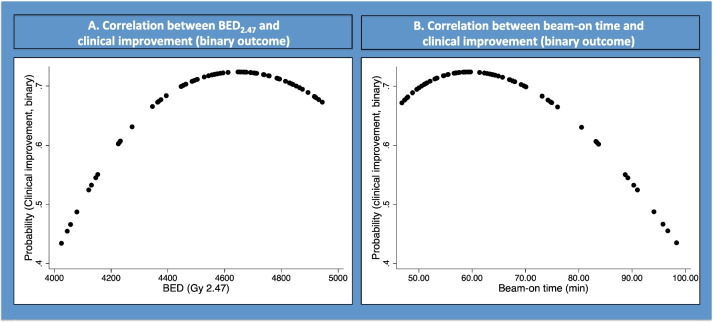
Stereotactic radiosurgery (SRS) is one of the surgical alternatives for drug-resistant essential tremor (ET). Here, we aimed at evaluating whether biologically effective dose (BEDGy2.47) is relevant for tremor improvement after stereotactic radiosurgical thalamotomy in a population of patients treated with one (unplugged) isocenter and a uniform dose of 130 Gy. This is a retrospective longitudinal single center study. Seventy-eight consecutive patients were clinically analyzed. Mean age was 69.1 years (median 71, range 36-88). Mean follow-up period was 14 months (median 12, 3-36). Tremor improvement was assessed at 12 months after SRS using the ET rating assessment scale (TETRAS, continuous outcome) and binary (binary outcome). BED was defined for an alpha/beta of 2.47, based upon previous studies considering such a value for the normal brain. Mean BED was 4573.1 Gy2.47 (median 4612, 4022.1-4944.7). Mean beam-on time was 64.7 min (median 61.4; 46.8-98.5). There was a statically significant correlation between delta (follow-up minus baseline) in TETRAS (total) with BED (p = 0.04; beta coefficient - 0.029) and beam-on time (p = 0.03; beta coefficient 0.57) but also between TETRAS (ADL) with BED (p = 0.02; beta coefficient 0.038) and beam-on time (p = 0.01; beta coefficient 0.71). Fractional polynomial multivariate regression suggested that a BED > 4600 Gy2.47 and a beam-on time > 70 min did not further increase clinical efficacy (binary outcome). Adverse radiation events (ARE) were defined as larger MR signature on 1-year follow-up MRI and were present in 7 out of 78 (8.9%) cases, receiving a mean BED of 4650 Gy2.47 (median 4650, range 4466-4894). They were clinically relevant with transient hemiparesis in 5 (6.4%) patients, all with BED values higher than 4500 Gy2.47. Tremor improvement was correlated with BED Gy2.47 after SRS for drug-resistant ET. An optimal BED value for tremor improvement was 4300-4500 Gy2.47. ARE appeared for a BED of more than 4500 Gy2.47. Such finding should be validated in larger cohorts.
Keywords: Biologically effective dose; Essential tremor; Radiosurgery; TETRAS.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Berger A, Alzate JD, Bernstein K, Mullen R, McMenomey S, Jethanemest D, Friedmann DR, Smouha E, Sulman EP, Silverman JS, Roland JT, Golfinos JG, Kondziolka D (2022) Modern hearing preservation outcomes after vestibular schwannoma stereotactic radiosurgery. Neurosurgery 91:648–657. 10.1227/neu.0000000000002090 - DOI - PMC - PubMed
-
- Blomstedt Y, Stenmark Persson R, Awad A, Hariz GM, Philipson J, Hariz M, Fytagoridis A, Blomstedt P (2023) 10 Years follow-up of deep brain stimulation in the caudal zona incerta/posterior subthalamic area for essential tremor. Mov Disord Clin Pract 10:783–793. 10.1002/mdc3.13729 - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
