

Determinants of lenalidomide response with or without erythropoiesis-stimulating agents in myelodysplastic syndromes: the HOVON89 trial
- PMID: 38297135
- PMCID: PMC10997501
- DOI: 10.1038/s41375-024-02161-6
Determinants of lenalidomide response with or without erythropoiesis-stimulating agents in myelodysplastic syndromes: the HOVON89 trial
Abstract
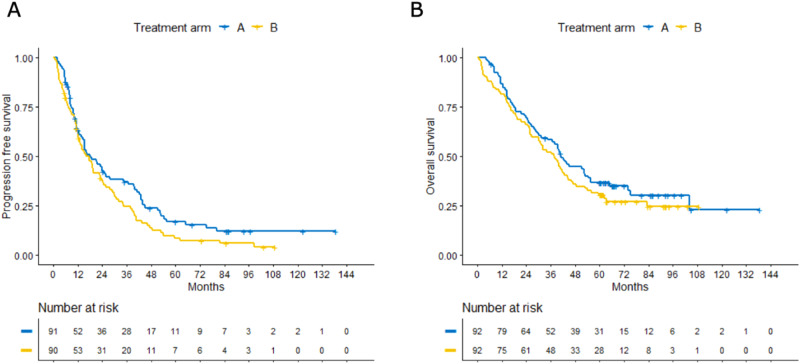
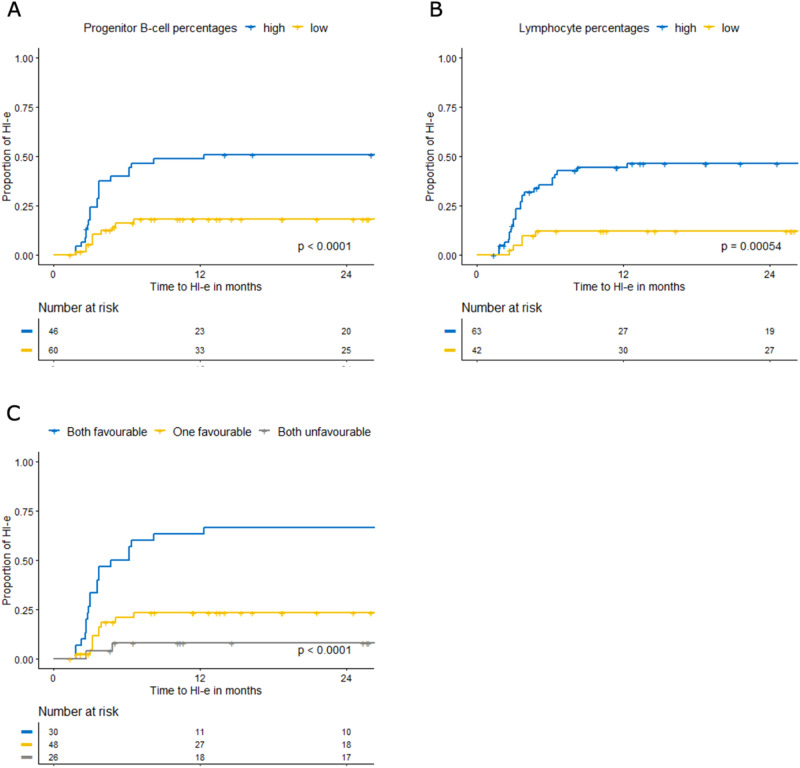
A randomized phase-II study was performed in low/int-1 risk MDS (IPSS) to study efficacy and safety of lenalidomide without (arm A) or with (arm B) ESA/G-CSF. In arm B, patients without erythroid response (HI-E) after 4 cycles received ESA; G-CSF was added if no HI-E was obtained by cycle 9. HI-E served as primary endpoint. Flow cytometry and next-generation sequencing were performed to identify predictors of response. The final evaluation comprised 184 patients; 84% non-del(5q), 16% isolated del(5q); median follow-up: 70.7 months. In arm A and B, 39 and 41% of patients achieved HI-E; median time-to-HI-E: 3.2 months for both arms, median duration of-HI-E: 9.8 months. HI-E was significantly lower in non-del(5q) vs. del(5q): 32% vs. 80%. The same accounted for transfusion independency-at-week 24 (16% vs. 67%), but similar in both arms. Apart from presence of del(5q), high percentages of bone marrow lymphocytes and progenitor B-cells, a low number of mutations, absence of ring sideroblasts, and SF3B1 mutations predicted HI-E. In conclusion, lenalidomide induced HI-E in patients with non-del(5q) and del(5q) MDS without additional effect of ESA/G-CSF. The identified predictors of response may guide application of lenalidomide in lower-risk MDS in the era of precision medicine. (EudraCT 2008-002195-10).
© 2024. The Author(s).
Conflict of interest statement
AL: research support: Celgene/BMS, Roche, Alexion; advisory boards: Celgene/BMS, Amgen, Novartis, Pfizer, AbbVie, Syros; speakers fee: Celgene/BMS, Novartis, Takeda. PM: advisory boards: Novartis; speakers fee: Sobi. PB: advisory boards: AbbVie; speakers fee: Novartis. JJ: research support: Novartis, BMS. President, Apps for Care and Science, nonprofit. foundation supported by Amgen, Astellas, Daiichi-Sankyo, Janssen, Olympus, Incyte, BMS, Sanofi Genzyme, Servier, Jazz, Takeda. Honoraria: Abbvie, Novartis, Pfizer, Incyte. All other authors declared no conflicts of interest.
Figures


References
-
- Park S, Greenberg P, Yucel A, Farmer C, O’Neill F, De Oliveira Brandao C, et al. Clinical effectiveness and safety of erythropoietin-stimulating agents for the treatment of low- and intermediate-1-risk myelodysplastic syndrome: a systematic literature review. Br J Haematol. 2019;184:134–60. doi: 10.1111/bjh.15707. - DOI - PubMed
-
- Fenaux P, Giagounidis A, Selleslag D, Beyne-Rauzy O, Mufti G, Mittelman M, et al. A randomized phase 3 study of lenalidomide versus placebo in RBC transfusion-dependent patients with Low-/Intermediate-1-risk myelodysplastic syndromes with del5q. Blood. 2011;118:3765–76. doi: 10.1182/blood-2011-01-330126. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
