Alcohol-associated liver disease
- PMID: 38299591
- PMCID: PMC10836812
- DOI: 10.1172/JCI176345
Alcohol-associated liver disease
Abstract
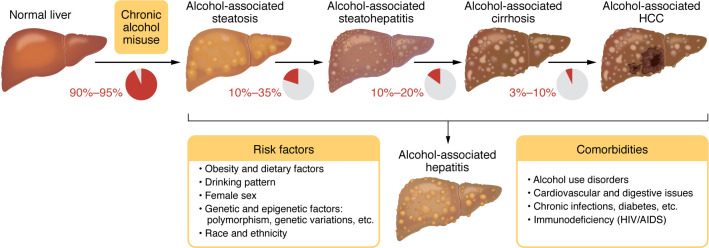
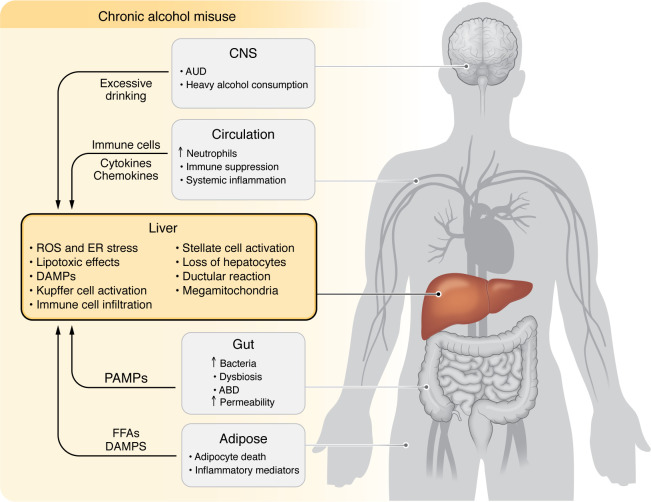
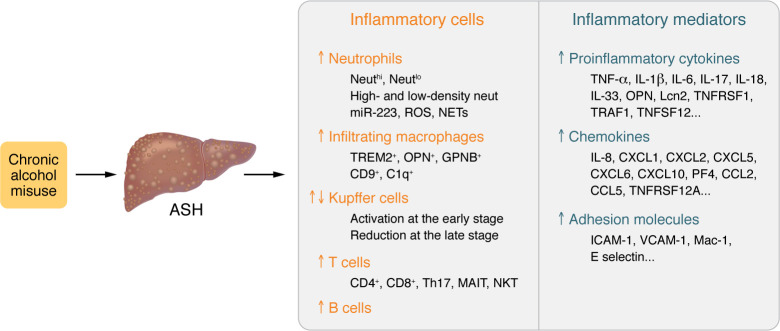
Alcohol-associated liver disease (ALD) is a major cause of chronic liver disease worldwide, and comprises a spectrum of several different disorders, including simple steatosis, steatohepatitis, cirrhosis, and superimposed hepatocellular carcinoma. Although tremendous progress has been made in the field of ALD over the last 20 years, the pathogenesis of ALD remains obscure, and there are currently no FDA-approved drugs for the treatment of ALD. In this Review, we discuss new insights into the pathogenesis and therapeutic targets of ALD, utilizing the study of multiomics and other cutting-edge approaches. The potential translation of these studies into clinical practice and therapy is deliberated. We also discuss preclinical models of ALD, interplay of ALD and metabolic dysfunction, alcohol-associated liver cancer, the heterogeneity of ALD, and some potential translational research prospects for ALD.
Figures