

Atypia detected during breast screening and subsequent development of cancer: observational analysis of the Sloane atypia prospective cohort in England
- PMID: 38302129
- PMCID: PMC10831586
- DOI: 10.1136/bmj-2023-077039
Atypia detected during breast screening and subsequent development of cancer: observational analysis of the Sloane atypia prospective cohort in England
Abstract
Objective: To explore how the number and type of breast cancers developed after screen detected atypia compare with the anticipated 11.3 cancers detected per 1000 women screened within one three year screening round in the United Kingdom.
Design: Observational analysis of the Sloane atypia prospective cohort in England.
Setting: Atypia diagnoses through the English NHS breast screening programme reported to the Sloane cohort study. This cohort is linked to the English Cancer Registry and the Mortality and Birth Information System for information on subsequent breast cancer and mortality.
Participants: 3238 women diagnosed as having epithelial atypia between 1 April 2003 and 30 June 2018.
Main outcome measures: Number and type of invasive breast cancers detected at one, three, and six years after atypia diagnosis by atypia type, age, and year of diagnosis.
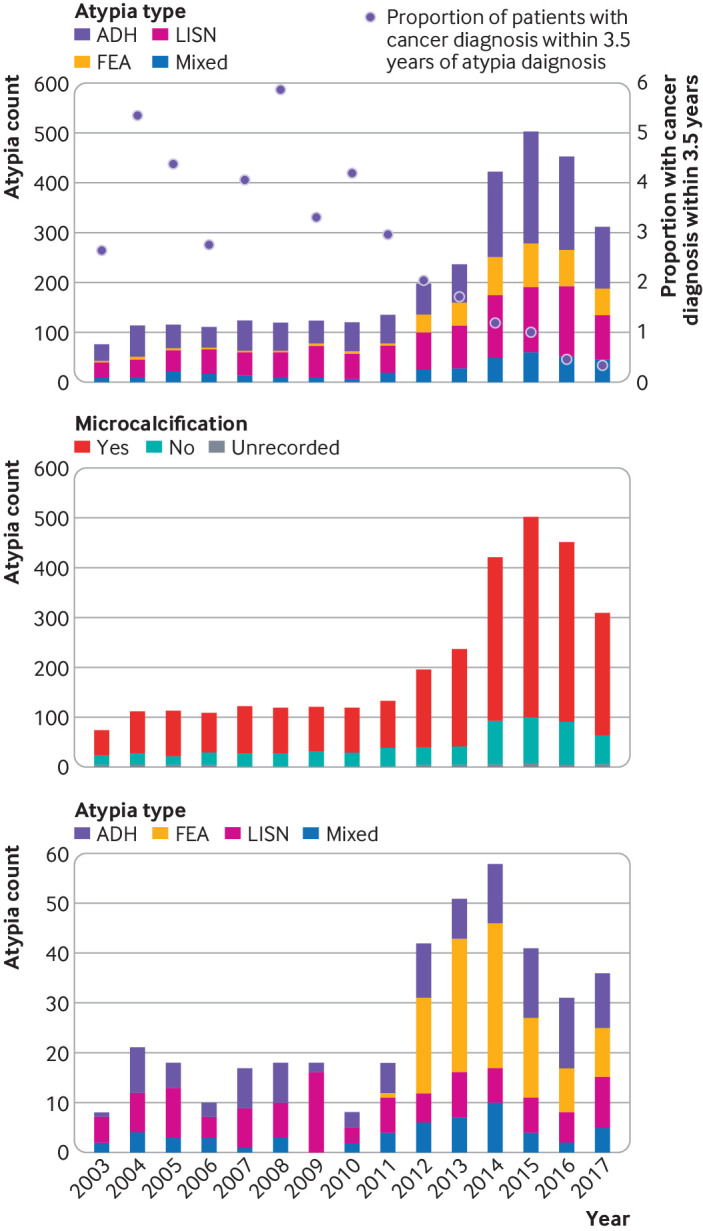
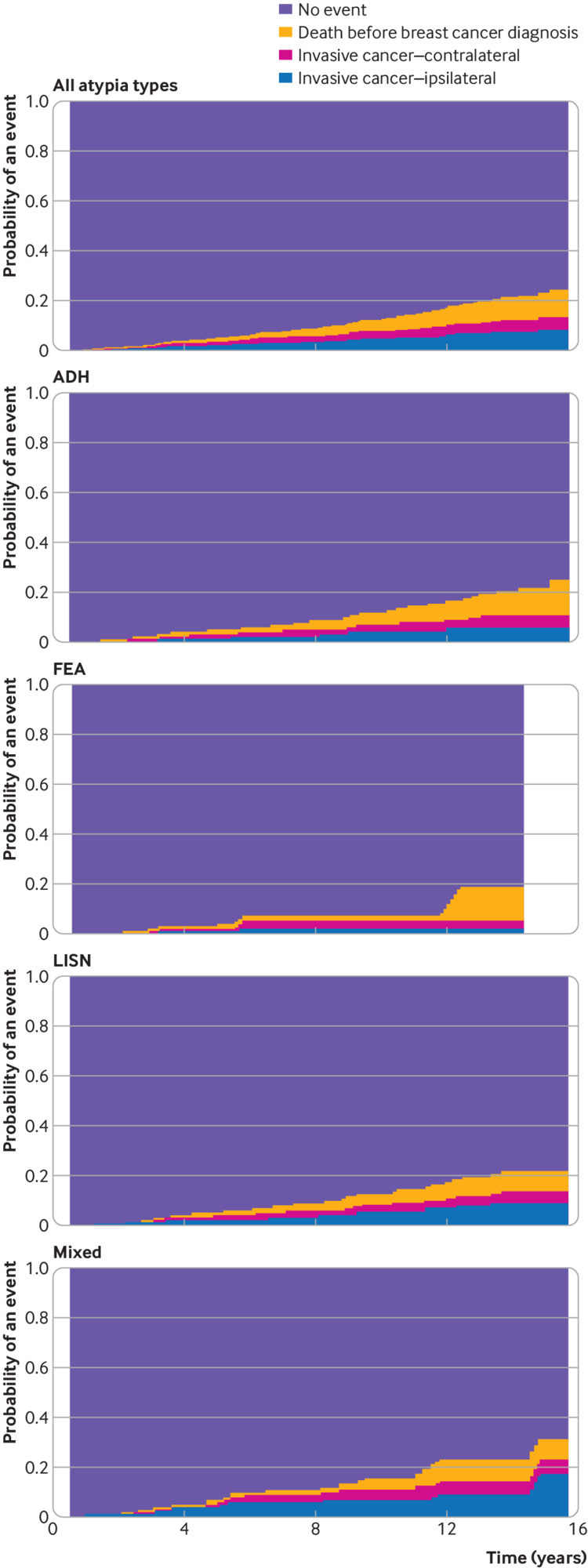
Results: There was a fourfold increase in detection of atypia after the introduction of digital mammography between 2010 (n=119) and 2015 (n=502). During 19 088 person years of follow-up after atypia diagnosis (until December 2018), 141 women developed breast cancer. Cumulative incidence of cancer per 1000 women with atypia was 0.95 (95% confidence interval 0.28 to 2.69), 14.2 (10.3 to 19.1), and 45.0 (36.3 to 55.1) at one, three, and six years after atypia diagnosis, respectively. Women with atypia detected more recently have lower rates of subsequent cancers detected within three years (6.0 invasive cancers per 1000 women (95% confidence interval 3.1 to 10.9) in 2013-18 v 24.3 (13.7 to 40.1) in 2003-07, and 24.6 (14.9 to 38.3) in 2008-12). Grade, size, and nodal involvement of subsequent invasive cancers were similar to those of cancers detected in the general screening population, with equal numbers of ipsilateral and contralateral cancers.
Conclusions: Many atypia could represent risk factors rather than precursors of invasive cancer requiring surgery in the short term. Women with atypia detected more recently have lower rates of subsequent cancers detected, which might be associated with changes to mammography and biopsy techniques identifying forms of atypia that are more likely to represent overdiagnosis. Annual mammography in the short term after atypia diagnosis might not be beneficial. More evidence is needed about longer term risks.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/disclosure-of-interest/ and declare: support from National Institute for Health and Care Research (NIHR) Research for Patient Benefit Call (RfPB) for the submitted work. KF, DJ, STP, NSt, NSh, and SEP received funding from the NIHR RfPB for the conduct of this study. KF was funded by an NIHR Development and Skills Enhancement award (NIHR302371). STP is funded by the NIHR through a research professorship (NIHR302434). EP received speaker’s honoraria and travel costs from Roche to speak at an advisory group meeting. KC is funded as part of the Cancer Grand Challenges PRECISION team (C38317/A24043) which is funded by Cancer Research UK and the Dutch Cancer Society. HS received travel and support to attend meetings of CRUK Grand Challenge Precision. SEP and AMT are members of the PRECISION Consortium, a recipient of a Cancer Research UK Grand Challenge Award, jointly funded by Cancer Research UK and the Dutch Cancer Society (KWF). AMS has participated in advisory boards for Exact Sciences and Veracyte. BH, MGW, OK, and CCK have nothing to declare.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous