

Systematic pulmonary embolism follow-up increases diagnostic rates of chronic thromboembolic pulmonary hypertension and identifies less severe disease: results from the ASPIRE Registry
- PMID: 38302154
- PMCID: PMC7615743
- DOI: 10.1183/13993003.00846-2023
Systematic pulmonary embolism follow-up increases diagnostic rates of chronic thromboembolic pulmonary hypertension and identifies less severe disease: results from the ASPIRE Registry
Abstract
Background: Diagnostic rates and risk factors for the subsequent development of chronic thromboembolic pulmonary hypertension (CTEPH) following pulmonary embolism (PE) are not well defined.
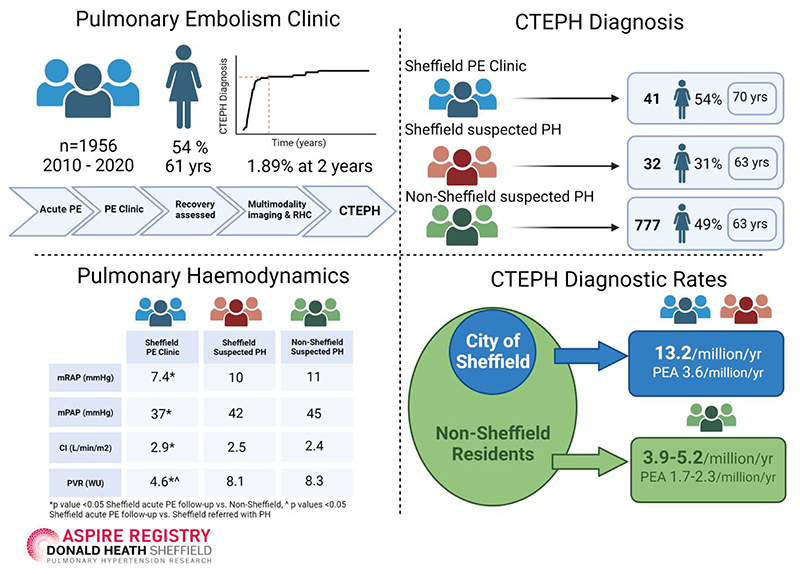
Methods: Over a 10-year period (2010-2020), consecutive patients attending a PE follow-up clinic in Sheffield, UK (population 554 600) and all patients diagnosed with CTEPH at a pulmonary hypertension (PH) referral centre in Sheffield (referral population estimated 15-20 million) were included.
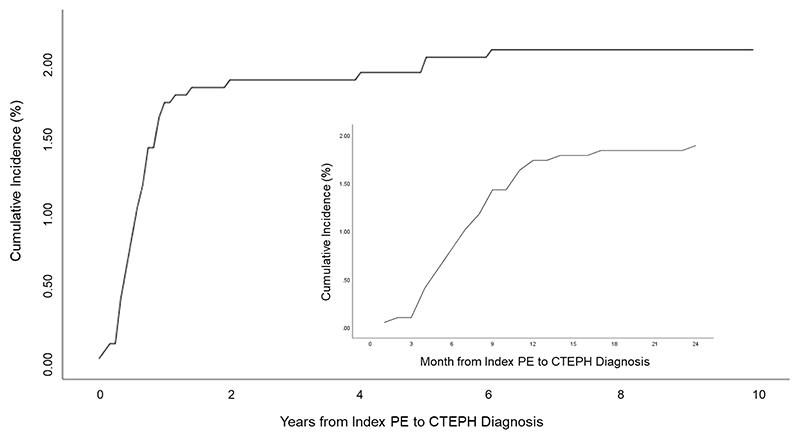
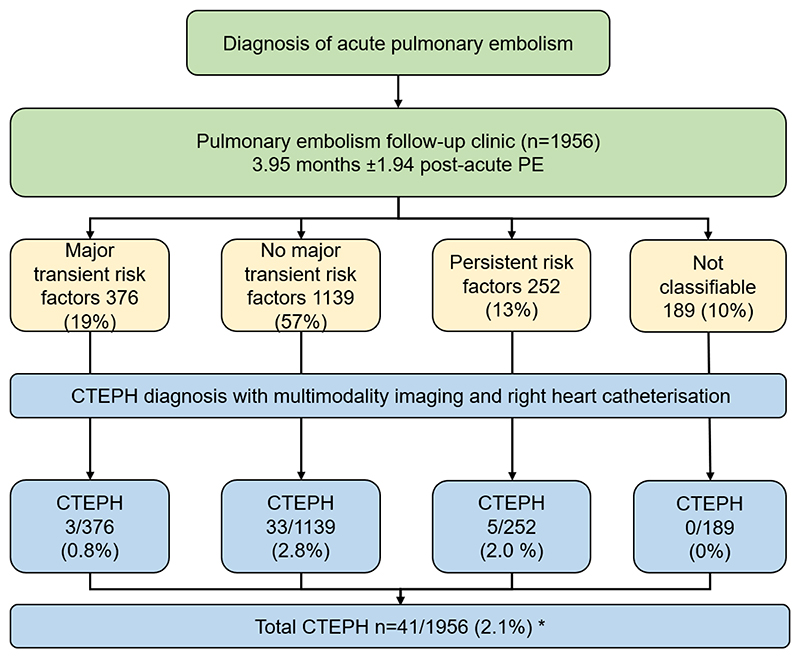
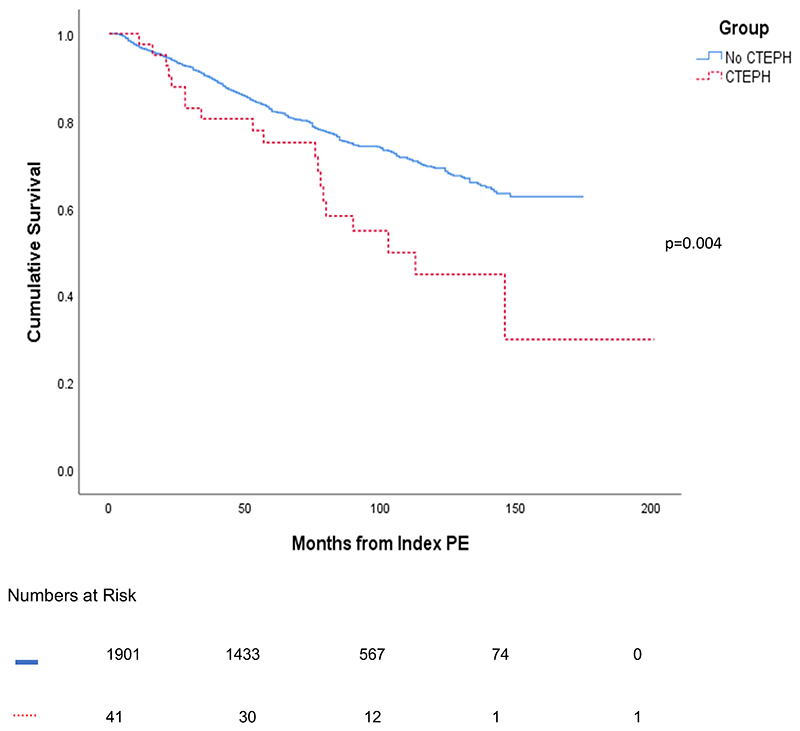
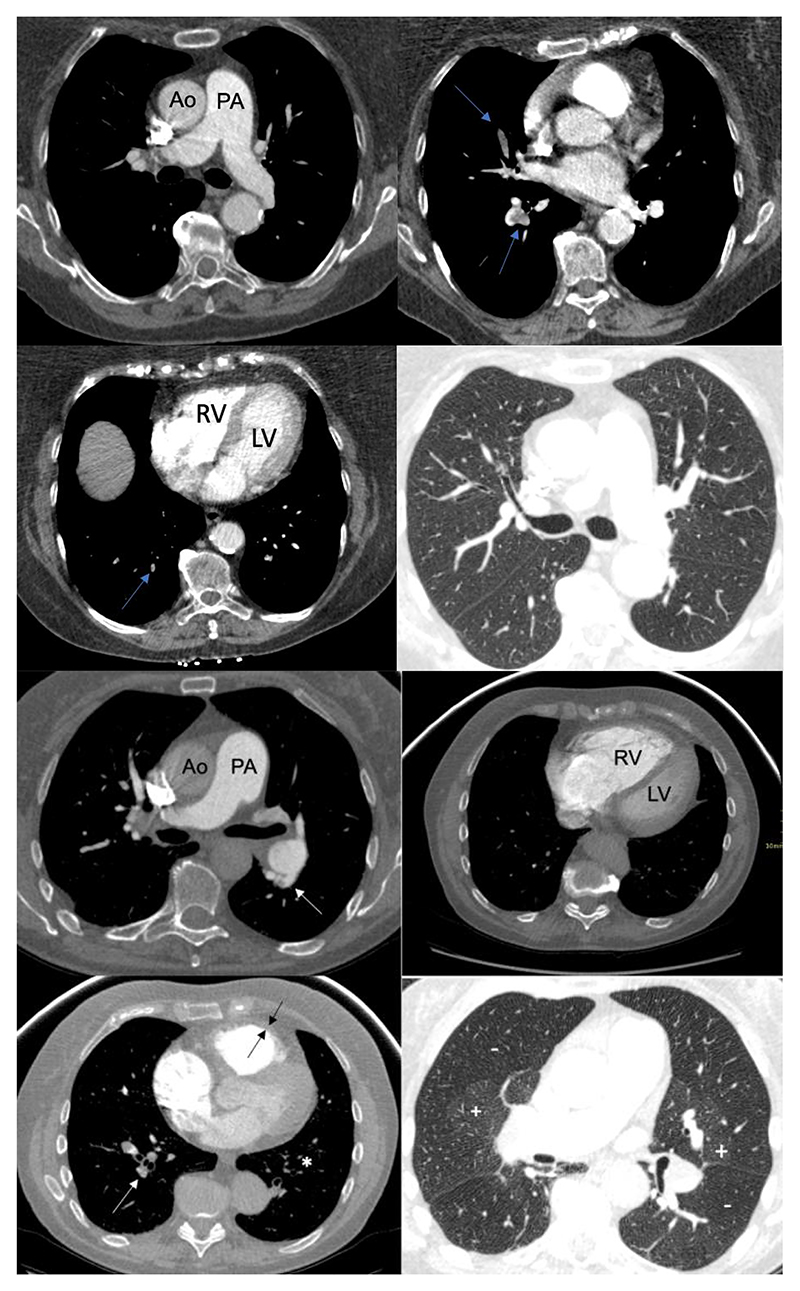
Results: Of 1956 patients attending the Sheffield PE clinic 3 months following a diagnosis of acute PE, 41 were diagnosed with CTEPH with a cumulative incidence of 2.10%, with 1.89% diagnosed within 2 years. Of 809 patients presenting with pulmonary hypertension (PH) and diagnosed with CTEPH, 32 were Sheffield residents and 777 were non-Sheffield residents. Patients diagnosed with CTEPH at the PE follow-up clinic had shorter symptom duration (p<0.01), better exercise capacity (p<0.05) and less severe pulmonary haemodynamics (p<0.01) compared with patients referred with suspected PH. Patients with no major transient risk factors present at the time of acute PE had a significantly higher risk of CTEPH compared with patients with major transient risk factors (OR 3.6, 95% CI 1.11-11.91; p=0.03). The presence of three computed tomography (CT) features of PH in combination with two or more out of four features of chronic thromboembolic pulmonary disease at the index PE was found in 19% of patients who developed CTEPH and in 0% of patients who did not. Diagnostic rates and pulmonary endarterectomy (PEA) rates were higher at 13.2 and 3.6 per million per year, respectively, for Sheffield residents compared with 3.9-5.2 and 1.7-2.3 per million per year, respectively, for non-Sheffield residents.
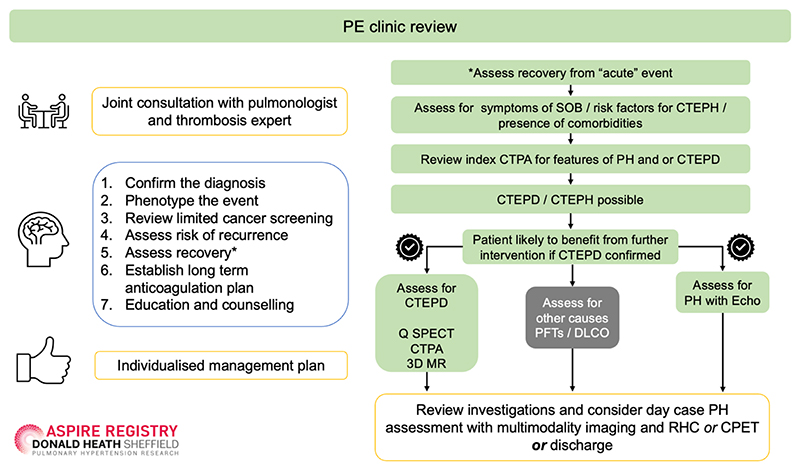
Conclusions: In the real-world setting a dedicated PE follow-up pathway identifies patients with less severe CTEPH and increases population-based CTEPH diagnostic and PEA rates. At the time of acute PE diagnosis the absence of major transient risk factors, CT features of PH and chronic thromboembolism are risk factors for a subsequent diagnosis of CTEPH.
Copyright ©The authors 2024. For reproduction rights and permissions contact permissions@ersnet.org.
Conflict of interest statement
Conflict of interest: C. Durrington reports support for the present manuscript from NIHR Sheffield Biomedical Research Centre, and also reports lecture honoraria from Janssen Pharmaceuticals, outside the submitted work. C.A. Elliot reports lecture honoraria and travel support from Janssen Pharmaceuticals, outside the submitted work. D. De-Fonseka reports a leadership role on the Pleural Specialist Advisory Group and Pleural Disease Guideline Committee for the British Thoracic Society, outside the submitted work. A.J. Swift reports support for the present manuscript from a Wellcome Trust fellowship, and also reports grants from Janssen Pharmaceuticals, NIHR and Wellcome Trust, and consulting fees from Janssen Pharmaceuticals, outside the submitted work. K. Dwivedi reports support for the present manuscript from Wellcome 4Ward North fellowship, and also reports grants from Janssen, and lecture honoraria from Royal College of Radiologists, and is a committee member for the Royal College of Radiologists Artificial Intelligence Working Group and Royal College of Radiologists RADIANT group, outside the submitted work. A. Charalampopoulos reports lecture honoraria from Janssen and Boehringer, outside the submitted work. A. Hameed reports lecture honoraria and travel support from Janssen, outside the submitted work. A.M.K. Rothman reports grants from a Wellcome Trust Clinical Research Career Development Fellowship (206632/Z/17/Z), MRC (experimental medicine grant MR/W026279/1), Abbott Laboratories, Medtronic Inc., Endotronix, SoniVie, NXT Biomedical, Gradient and Neptune Medical, outside the submitted work. N. Hamilton reports consulting fees and travel support from Janssen, lecture honoraria from MSD and Janssen, advisory board participation with Bayer, MSD, Janssen and Vifor, and a leadership role as pharmacist for the NHS Specialist Respiratory Clinical Reference Group, outside the submitted work. A.A.R. Thompson reports grants from the British Heart Foundation and NIHR, and lecture honoraria and travel support from Janssen-Cilag Ltd, outside the submitted work. R. Condliffe reports lecture honoraria and travel support from Janssen Pharmaceuticals, outside the submitted work. D.G. Kiely reports support for the present manuscript from NIHR Sheffield Biomedical Research Centre, and also reports grants from Janssen Pharmaceuticals, NIHR Sheffield Biomedical Research Centre and Ferrer, consulting fees and lecture honoraria from Janssen Pharmaceuticals, Ferrer, Altavant, MSD and United Therapeutics, travel support from Janssen, Ferrer, MSD and United Therapeutics, advisory board membership for Janssen and MSD, and leadership roles as a member of the Clinical Reference Group for Specialised Respiratory Medicine (NHS England) and lead of the UK National Audit of Pulmonary Hypertension, outside the submitted work. The remaining authors have no potential conflicts of interest to disclose.
Figures
Comment in
-
Systematic pulmonary embolism follow-up: why we should all do it!Eur Respir J. 2024 Mar 14;63(3):2400253. doi: 10.1183/13993003.00253-2024. Print 2024 Mar. Eur Respir J. 2024. PMID: 38485183 No abstract available.
References
-
- Huisman Mv, Barco S, Cannegieter SC, le Gal G, Konstantinides Sv, Reitsma PH, Rodger M, Noordegraaf AV, Klok FA. Pulmonary embolism. Nat Rev Dis Primers. 2018;4:18028. - PubMed
-
- Goldhaber SZ, Visani L, De Rosa M. Acute pulmonary embolism: clinical outcomes in the International Cooperative Pulmonary Embolism Registry (ICOPER) Lancet. 1999;353:1386–1389. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical