

Durvalumab and guadecitabine in advanced clear cell renal cell carcinoma: results from the phase Ib/II study BTCRC-GU16-043
- PMID: 38302476
- PMCID: PMC10834488
- DOI: 10.1038/s41467-024-45216-z
Durvalumab and guadecitabine in advanced clear cell renal cell carcinoma: results from the phase Ib/II study BTCRC-GU16-043
Abstract
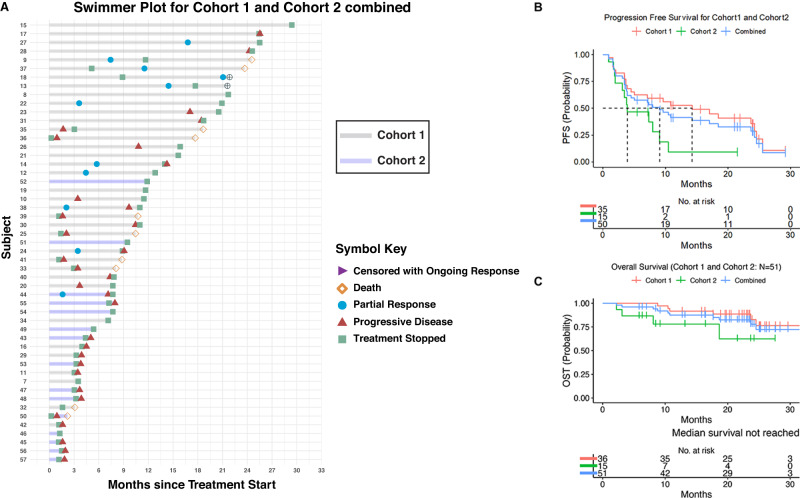
Epigenetic modulation is well established in hematologic malignancies but to a lesser degree in solid tumors. Here we report the results of a phase Ib/II study of guadecitabine and durvalumab in advanced clear cell renal cell carcinoma (ccRCC; NCT03308396). Patients received guadecitabine (starting at 60 mg/m2 subcutaneously on days 1-5 with de-escalation to 45 mg/m2 in case of dose limiting toxicity) with durvalumab (1500 mg intravenously on day 8). The study enrolled 57 patients, 6 in phase Ib with safety being the primary objective and 51in phase II, comprising 2 cohorts: 36 patients in Cohort 1 were treatment naive to checkpoint inhibitors (CPI) with 0-1 prior therapies and 15 patients in Cohort 2 were treated with up to two prior systemic therapies including one CPI. The combination of guadecitabine 45 mg/m2 with durvalumab 1500 mg was deemed safe. The primary objective of overall response rate (ORR) in cohort 1 was 22%. Sixteen patients (44%) experienced stable disease (SD). Secondary objectives included overall survival (OS), duration of response, progression-free survival (PFS), clinical benefit rate, and safety as well as ORR for Cohort 2. Median PFS for cohort 1 and cohort 2 were 14.26 and 3.91 months respectively. Median OS was not reached. In cohort 2, one patient achieved a partial response and 60% achieved SD. Asymptomatic neutropenia was the most common adverse event. Even though the trial did not meet the primary objective in cohort 1, the tolerability and PFS signal in CPI naive patients are worth further investigation.
© 2024. The Author(s).
Conflict of interest statement
Y.Z.: advisory boards: Bristol Myers Squibb, Amgen, Roche Diagnostics, Novartis, Janssen, Eisai, Exelixis, Castle Bioscience, Genzyme Corporation, Astrazeneca, Array, Bayer, Pfizer, Clovis, EMD Serono, Myovant. Grant/research support from: institutional clinical trial support from NewLinkGenetics, Pfizer, Exelixis, Eisai. Data safety and monitoring committee: Janssen Research and Development. Consultant honorarium: Pfizer, Novartis. E.S.: institutional research funding: Medivation/Astellas. Advisory boards: Merck, Johnson & Johnson, Vyriad. Data safety monitoring board: Aura Biosciences. M.J.: institutional research funding: AstraZeneca. Advisory boards: Seagen, Gilead. Travel and accommodation: DAVA Oncology. Mentor on diversity grant: Bristol Myers Squibb. S.A., R.H., D.P., V.B., A.M., XL, C.L., I.K., W.Z., A.A.: declare no competing interest.
Figures
References
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
