

Outpatient hysteroscopy impact on subsequent assisted reproductive technology: a systematic review and meta-analysis in patients with normal transvaginal sonography or hysterosalpingography images
- PMID: 38302947
- PMCID: PMC10832084
- DOI: 10.1186/s12958-024-01191-0
Outpatient hysteroscopy impact on subsequent assisted reproductive technology: a systematic review and meta-analysis in patients with normal transvaginal sonography or hysterosalpingography images
Abstract
Background: Standard management for intrauterine lesions typically involves initial imaging followed by operative hysteroscopy for suspicious findings. However, the efficacy of routine outpatient hysteroscopy in women undergoing assisted reproductive technology (ART) remains uncertain due to a lack of decisive high-quality evidence. This study aimed to determine whether outpatient hysteroscopy is beneficial for infertile women who have unremarkable imaging results prior to undergoing ART.
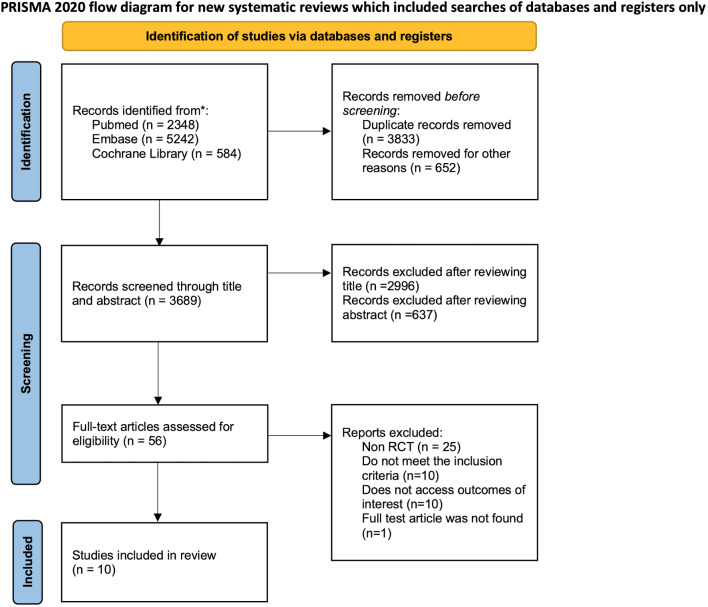
Methods: A systematic review and meta-analysis were conducted following PRISMA guidelines, incorporating data up to May 31, 2023, from databases such as PubMed, Embase, and the Cochrane Library. The primary outcome assessed was the live birth rate, with secondary outcomes including chemical pregnancy, clinical pregnancy rates, and miscarriage rates. Statistical analysis involved calculating risk ratios with 95% confidence intervals and assessing heterogeneity with the I2 statistic.
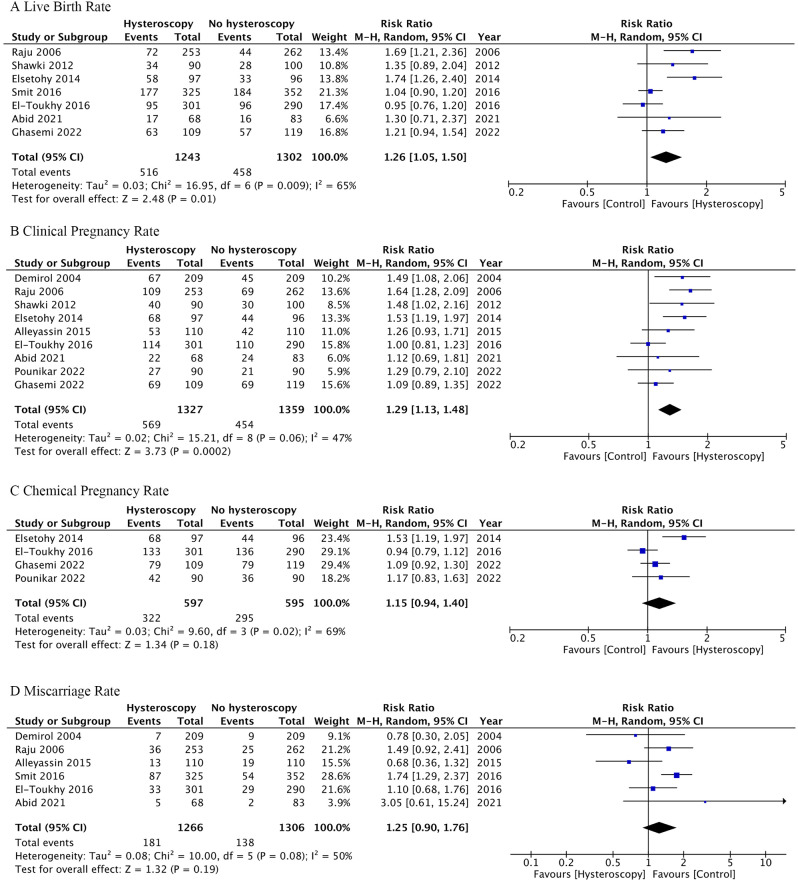
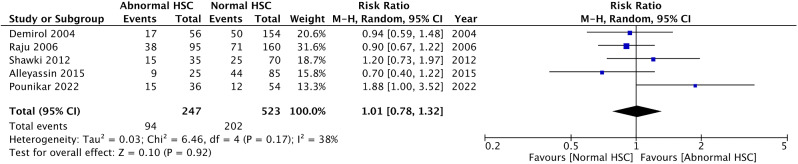
Results: The analysis included ten randomized control trials. Receiving outpatient hysteroscopy before undergoing ART was associated with increased live birth (RR 1.22, 95% CI 1.03-1.45, I2 61%) and clinical pregnancy rate (RR 1.27 95% CI 1.10-1.47, I2 53%). Miscarriage rates did not differ significantly (RR 1.25, CI 0.90-1.76, I2 50%). Subgroup analyses did not show a significant difference in clinical pregnancy rates when comparing normal versus abnormal hysteroscopic findings (RR 1.01, CI 0.78-1.32, I2 38%). We analyzed data using both intention-to-treat and per-protocol approaches, and our findings were consistent across both analytical methods.
Conclusions: Office hysteroscopy may enhance live birth and clinical pregnancy rates in infertile women undergoing ART, even when previous imaging studies show no apparent intrauterine lesions. Treating lesions not detected by imaging may improve ART outcomes. The most commonly missed lesions are endometrial polyps, submucosal fibroids and endometritis, which are all known to affect ART success rates. The findings suggested that hysteroscopy, given its diagnostic accuracy and patient tolerability, should be considered in the management of infertility.
Database registration: The study was registered in the International Prospective Register of Systemic Review database (CRD42023476403).
Keywords: Artificial reproductive technology; Diagnostic hysteroscopy; Hysterosalpingography; Infertility; Office hysteroscopy; Outpatient hysteroscopy; Transvaginal sonography; Transvaginal ultrasound.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- WHO. : Infertility Prevalence Estimates, 1990–2021. (Organization WH ed. Geneva; 2023.
-
- Practice Committee of the American Society for Reproductive M Effectiveness and treatment for unexplained infertility. Fertil Steril. 2006;86:111–4. doi: 10.1016/j.fertnstert.2006.07.1475. - DOI
-
- Domali E, Kyriakopoulos K, Antsaklis A. Ultrasonography: the Main Diagnostic Tool in Subfertile Women. Donald School Journal of Ultrasound in Obstetrics and Gynecology. 2012;6:270–85. doi: 10.5005/jp-journals-10009-1250. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
