

Effectiveness of Telemedicine for Musculoskeletal Disorders: Umbrella Review
- PMID: 38306156
- PMCID: PMC10873802
- DOI: 10.2196/50090
Effectiveness of Telemedicine for Musculoskeletal Disorders: Umbrella Review
Abstract
Background: Several systematic reviews (SRs) assessing the use of telemedicine for musculoskeletal conditions have been published in recent years. However, the landscape of evidence on multiple clinical outcomes remains unclear.
Objective: We aimed to summarize the available evidence from SRs on telemedicine for musculoskeletal disorders.
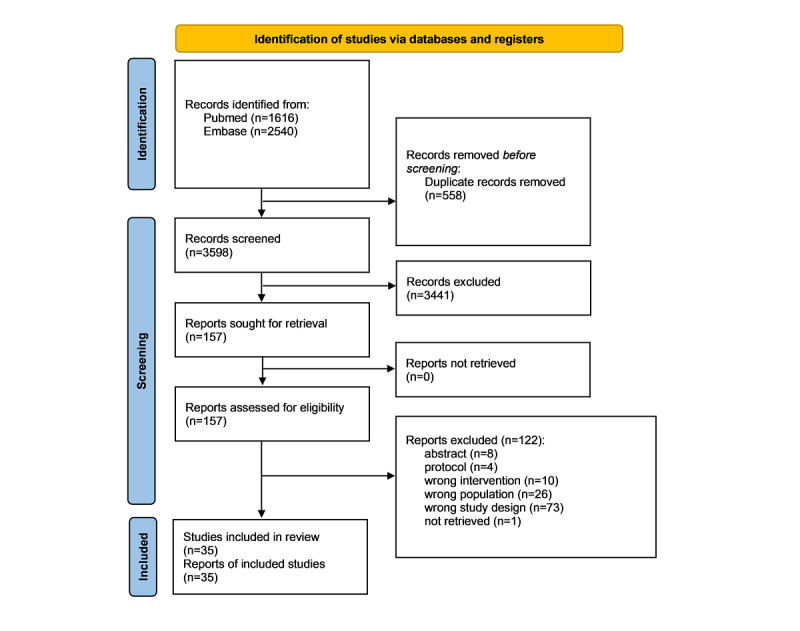
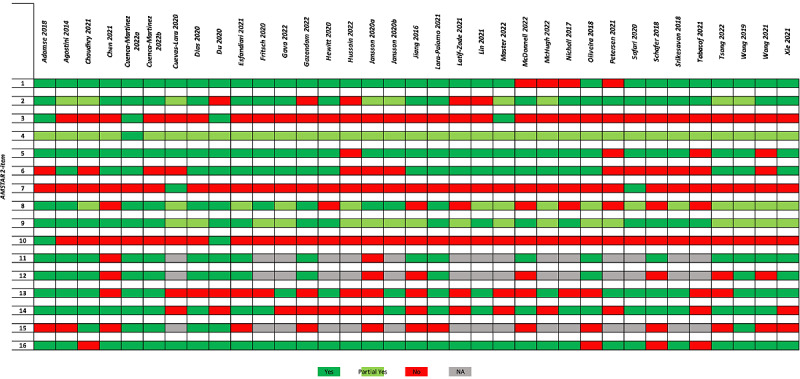
Methods: We conducted an umbrella review of SRs with and without meta-analysis by searching PubMed and EMBASE up to July 25, 2022, for SRs of randomized controlled trials assessing telemedicine. We collected any kind of patient-reported outcome measures (PROMs), patient-reported experience measures (PREMs), and objective measures, including direct and indirect costs. We assessed the methodological quality with the AMSTAR 2 tool (A Measurement Tool to Assess systematic Reviews 2). Findings were reported qualitatively.
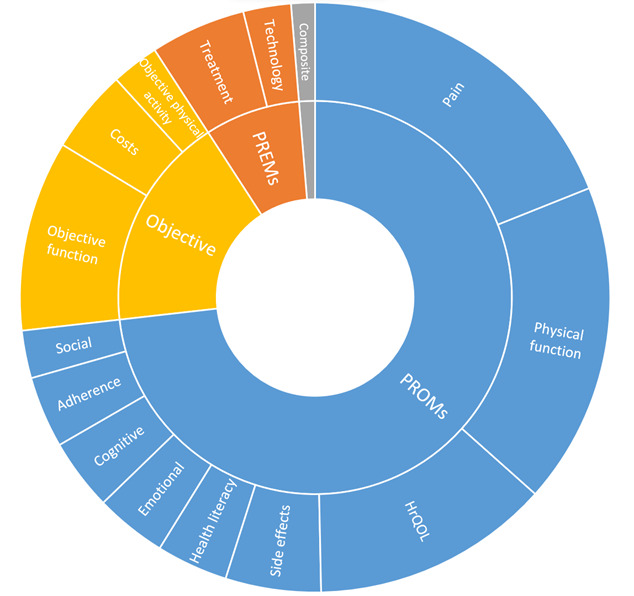
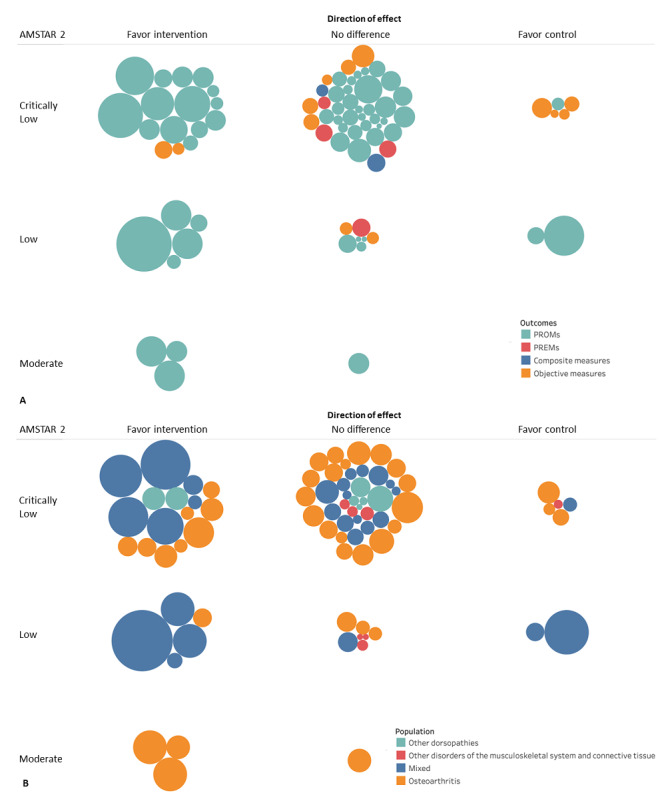
Results: Overall, 35 SRs published between 2015 and 2022 were included. Most reviews (n=24, 69%) were rated as critically low quality by AMSTAR 2. The majority of reviews assessed "telerehabilitation" (n=29) in patients with osteoarthritis (n=13) using PROMs (n=142 outcomes mapped with n=60 meta-analyses). A substantive body of evidence from meta-analyses found telemedicine to be beneficial or equal in terms of PROMs compared to conventional care (n=57 meta-analyses). Meta-analyses showed no differences between groups in PREMs (n=4), while objectives measures (ie, "physical function") were mainly in favor of telemedicine or showed no difference (9/13). All SRs showed notably lower costs for telemedicine compared to in-person visits.
Conclusions: Telemedicine can provide more accessible health care with noninferior results for various clinical outcomes in comparison with conventional care. The assessment of telemedicine is largely represented by PROMs, with some gaps for PREMs, objective measures, and costs.
Trial registration: PROSPERO CRD42022347366; https://osf.io/pxedm/.
Keywords: PREMs; PROMs; accessibility; condition; health care; meta-analyses; musculoskeletal; musculoskeletal disorder; orthopedics; osteoarthritis; patient-reported; patient-reported experience measures; patient-reported outcomes measures; rehabilitation; systematic review; telemedicine; telerehabilitation.
©Silvia Bargeri, Greta Castellini, Jacopo Antonino Vitale, Stefania Guida, Giuseppe Banfi, Silvia Gianola, Federico Pennestrì. Originally published in the Journal of Medical Internet Research (https://www.jmir.org), 02.02.2024.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
Similar articles
-
[Volume and health outcomes: evidence from systematic reviews and from evaluation of Italian hospital data].Epidemiol Prev. 2013 Mar-Jun;37(2-3 Suppl 2):1-100. Epidemiol Prev. 2013. PMID: 23851286 Italian.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2020 Jan 9;1(1):CD011535. doi: 10.1002/14651858.CD011535.pub3. Cochrane Database Syst Rev. 2020. Update in: Cochrane Database Syst Rev. 2021 Apr 19;4:CD011535. doi: 10.1002/14651858.CD011535.pub4. PMID: 31917873 Free PMC article. Updated.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2017 Dec 22;12(12):CD011535. doi: 10.1002/14651858.CD011535.pub2. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2020 Jan 9;1:CD011535. doi: 10.1002/14651858.CD011535.pub3. PMID: 29271481 Free PMC article. Updated.
-
Falls prevention interventions for community-dwelling older adults: systematic review and meta-analysis of benefits, harms, and patient values and preferences.Syst Rev. 2024 Nov 26;13(1):289. doi: 10.1186/s13643-024-02681-3. Syst Rev. 2024. PMID: 39593159 Free PMC article.
Cited by
-
Advancing Musculoskeletal Care Using AI and Digital Health Applications: A Review of Commercial Solutions.HSS J. 2025 May 30:15563316251341321. doi: 10.1177/15563316251341321. Online ahead of print. HSS J. 2025. PMID: 40458230 Free PMC article. Review.
-
Acceptance, Satisfaction, and Preference With Telemedicine During the COVID-19 Pandemic in 2021-2022: Survey Among Patients With Chronic Pain.JMIR Form Res. 2024 Apr 29;8:e53154. doi: 10.2196/53154. JMIR Form Res. 2024. PMID: 38684086 Free PMC article.
-
Patients' Experience With Evaluation by Both a Musculoskeletal Physician and Physical Therapist in the Same Digital Visit: Survey Study.JMIR Form Res. 2025 Mar 3;9:e66744. doi: 10.2196/66744. JMIR Form Res. 2025. PMID: 40030049 Free PMC article.
-
Effectiveness and Feasibility of Digital Pulmonary Rehabilitation in Patients Undergoing Lung Cancer Surgery: Systematic Review and Meta-Analysis.J Med Internet Res. 2024 Nov 11;26:e56795. doi: 10.2196/56795. J Med Internet Res. 2024. PMID: 39527799 Free PMC article.
-
Translating in-person care to telehealth: a secondary analysis of GP consultations on musculoskeletal conditions.BJGP Open. 2025 Apr 24;9(1):BJGPO.2024.0013. doi: 10.3399/BJGPO.2024.0013. Print 2025 Apr. BJGP Open. 2025. PMID: 39191481 Free PMC article.
References
-
- Cottrell MA, Russell TG. Telehealth for musculoskeletal physiotherapy. Musculoskelet Sci Pract. 2020 Aug;48:102193. doi: 10.1016/j.msksp.2020.102193. https://europepmc.org/abstract/MED/32560876 S2468-7812(20)30291-5 - DOI - PMC - PubMed
-
- Monaghesh E, Hajizadeh A. The role of telehealth during COVID-19 outbreak: a systematic review based on current evidence. BMC Public Health. 2020 Aug 01;20(1):1193. doi: 10.1186/s12889-020-09301-4. https://bmcpublichealth.biomedcentral.com/articles/10.1186/s12889-020-09... 10.1186/s12889-020-09301-4 - DOI - DOI - PMC - PubMed
-
- Bordas-Martinez J, Matéu Gómez Lluís, Cámara Menoyo David, López-Sánchez Marta, Santos S, Molina-Molina M, Planas Rosa. Patient-reported outcomes measures (PROMs) and patient-reported experience measures (PREMs) of COVID-19 telerehabilitation: Prospective pilot program. Medicine (Baltimore) 2022 Aug 05;101(31):e29639. doi: 10.1097/MD.0000000000029639. https://europepmc.org/abstract/MED/35945781 00005792-202208050-00075 - DOI - PMC - PubMed
-
- Foni NO, Costa LAV, Velloso LMR, Pedrotti CHS. Telemedicine: Is it a tool for orthopedics? Curr Rev Musculoskelet Med. 2020 Dec;13(6):797–801. doi: 10.1007/s12178-020-09680-6. https://europepmc.org/abstract/MED/33119841 10.1007/s12178-020-09680-6 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
