

A landscape of checkpoint blockade resistance in cancer: underlying mechanisms and current strategies to overcome resistance
- PMID: 38306161
- PMCID: PMC10841019
- DOI: 10.1080/15384047.2024.2308097
A landscape of checkpoint blockade resistance in cancer: underlying mechanisms and current strategies to overcome resistance
Abstract
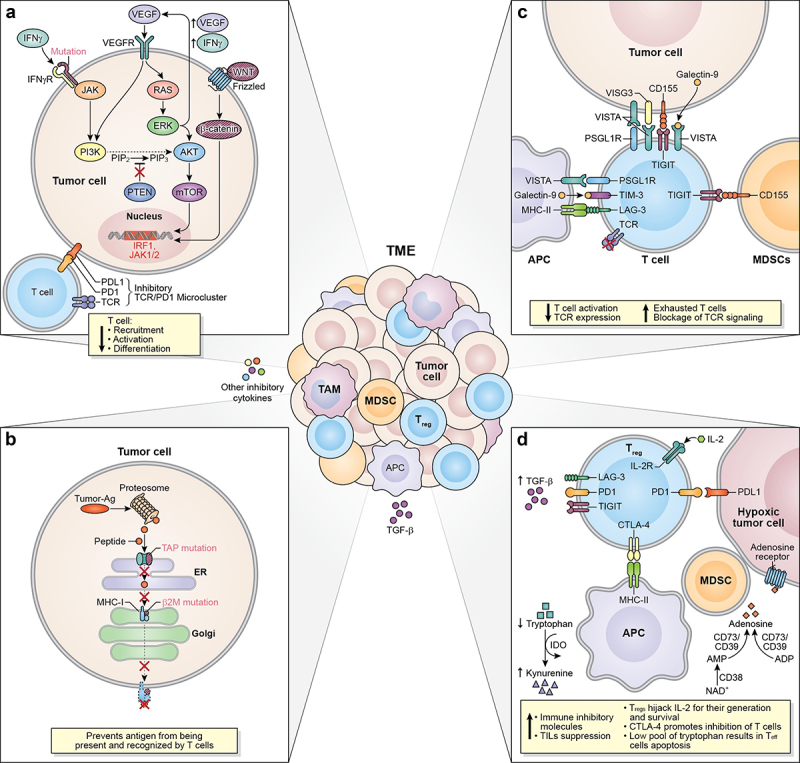
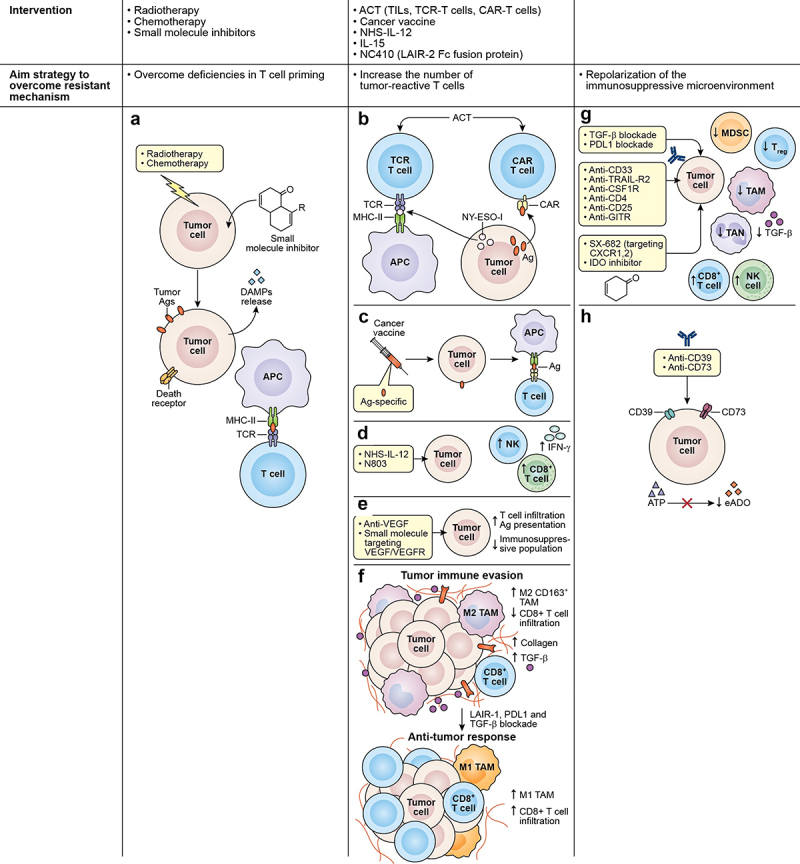
The discovery of immune checkpoints and the development of immune checkpoint inhibitors (ICI) have achieved a durable response in advanced-stage cancer patients. However, there is still a high proportion of patients who do not benefit from ICI therapy due to a lack of response when first treated (primary resistance) or detection of disease progression months after objective response is observed (acquired resistance). Here, we review the current FDA-approved ICI for the treatment of certain solid malignancies, evaluate the contrasting responses to checkpoint blockade in different cancer types, explore the known mechanisms associated with checkpoint blockade resistance (CBR), and assess current strategies in the field that seek to overcome these mechanisms. In order to improve current therapies and develop new ones, the immunotherapy field still has an unmet need in identifying other molecules that act as immune checkpoints, and uncovering other mechanisms that promote CBR.
Keywords: Immune checkpoint inhibitors (ICI); checkpoint blockade resistance; checkpoint blockade resistance mechanisms; immune checkpoint blockade; immunotherapy resistance.
Conflict of interest statement
No potential conflict of interest was reported by the author(s).
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous