

Implementation outcomes of the integrated district evidence to action (IDEAs) program to reduce neonatal mortality in central Mozambique: an application of the RE-AIM evaluation framework
- PMID: 38308300
- PMCID: PMC10835896
- DOI: 10.1186/s12913-024-10638-4
Implementation outcomes of the integrated district evidence to action (IDEAs) program to reduce neonatal mortality in central Mozambique: an application of the RE-AIM evaluation framework
Abstract
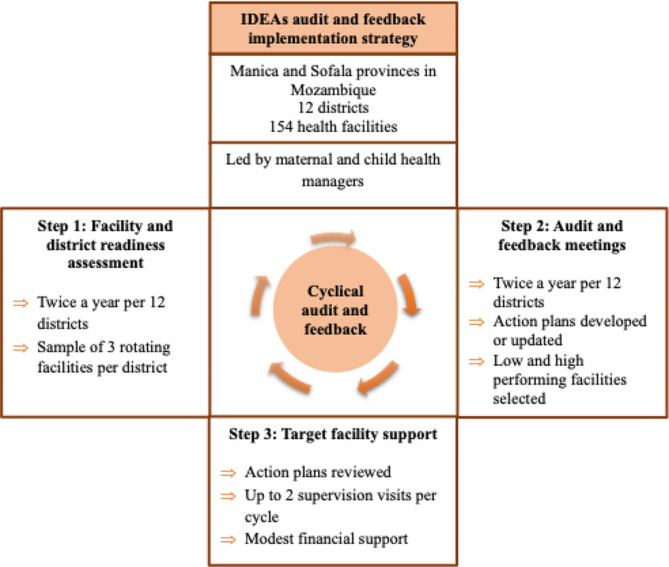
Background: Scarce evidence exists on audit and feedback implementation processes in low-resource health systems. The Integrated District Evidence to Action (IDEAs) is a multi-component audit and feedback strategy designed to improve the implementation of maternal and child guidelines in Mozambique. We report IDEAs implementation outcomes.
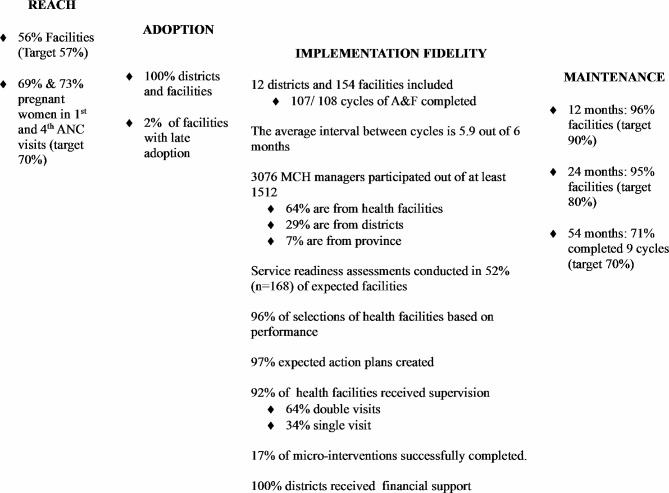
Methods: IDEAs was implemented in 154 health facilities across 12 districts in Manica and Sofala provinces between 2016 and 2020 and evaluated using a quasi-experimental design guided by the Reach, Effectiveness, Adoption, Implementation, and Maintenance (RE-AIM) framework. Reach is the proportion of pregnant women attending IDEAs facilities. Adoption is the proportion of facilities initiating audit and feedback meetings. Implementation is the fidelity to the strategy components, including readiness assessments, meetings (frequency, participation, action plan development), and targeted financial support and supervision. Maintenance is the sustainment at 12, 24, and 54 months.
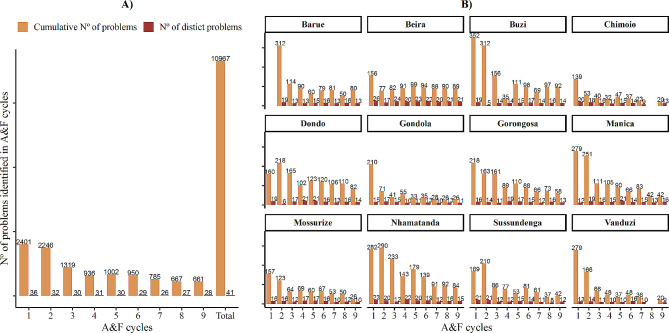
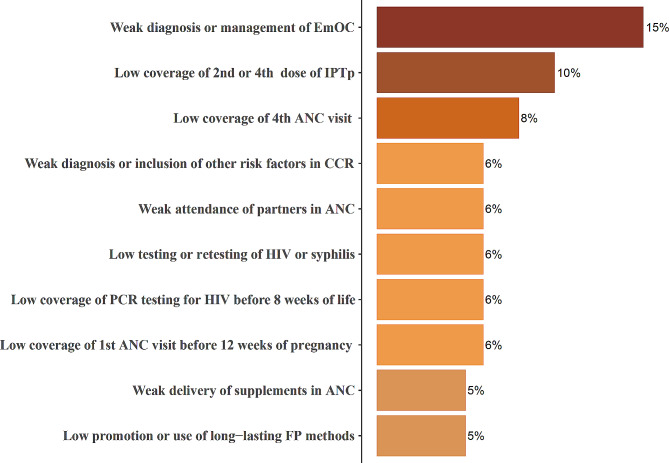
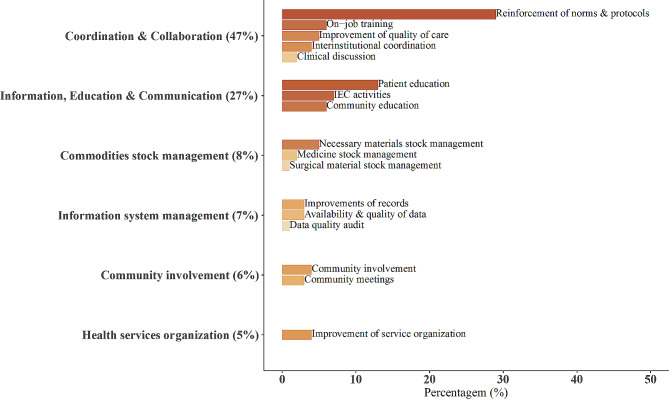
Results: Across both provinces, 56% of facilities were exposed to IDEAs (target 57%). Sixty-nine and 73% of pregnant women attended those facilities' first and fourth antenatal consultations (target 70%). All facilities adopted the intervention. 99% of the expected meetings occurred with an average interval of 5.9 out of 6 months. Participation of maternal and child managers was high, with 3076 attending meetings, of which 64% were from the facility, 29% from the district, and 7% from the province level. 97% of expected action plans were created, and 41 specific problems were identified. "Weak diagnosis or management of obstetric complications" was identified as the main problem, and "actions to reinforce norms and protocols" was the dominant subcategory of micro-interventions selected. Fidelity to semiannual readiness assessments was low (52% of expected facilities), and in completing micro-interventions (17% were completed). Ninety-six and 95% of facilities sustained the intervention at 12 and 24 months, respectively, and 71% had completed nine cycles at 54 months.
Conclusion: Maternal and child managers can lead audit and feedback processes in primary health care in Mozambique with high reach, adoption, and maintenance. The IDEAs strategy should be adapted to promote higher fidelity around implementing action plans and conducting readiness assessments. Adding effectiveness to these findings will help to inform strategy scale-up.
Keywords: Audit & Feedback; Health Systems Research; Implementation outcomes; Implementation science; Maternal and Child Health; Mozambique; Neonatal mortality; RE-AIM.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- United Nations Inter-agency Group for Child Mortality Estimation. Levels and trends in child mortality: report 2021. New York: United Nations Children’s Fund.; 2021. https://www.who.int/publications/m/item/levels-and-trends-in-child-morta.... Accessed 8 Mar 2023.
-
- Gülmezoglu AM, Lawrie TA, Hezelgrave N, Oladapo OT, Souza JP, Gielen M, Lawn JE, Bahl R, Althabe F, Colaci D, Hofmeyr GJ. Interventions to Reduce Maternal and Newborn Morbidity and Mortality. Reproductive, Maternal, Newborn, and Child Health.:115. 10.1596/978-1-4648-0348-2_ch7.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
