

Combining OPM and lesion mapping data for epilepsy surgery planning: a simulation study
- PMID: 38311614
- PMCID: PMC10838931
- DOI: 10.1038/s41598-024-51857-3
Combining OPM and lesion mapping data for epilepsy surgery planning: a simulation study
Abstract
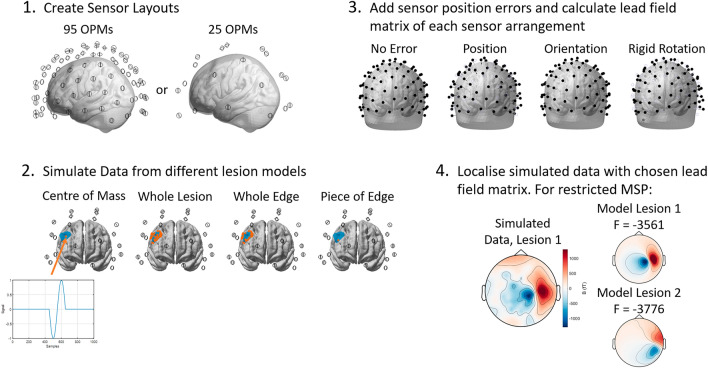
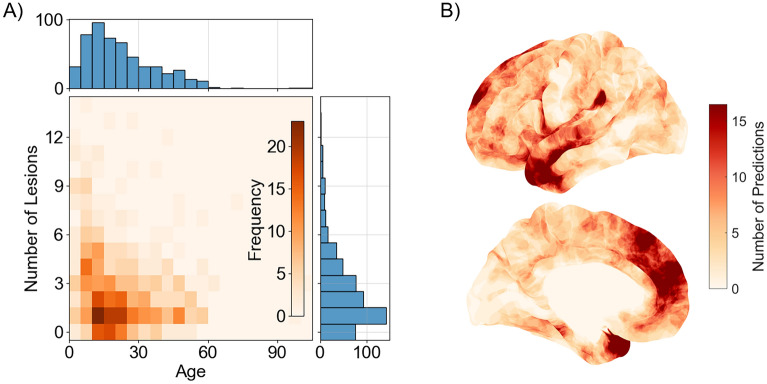
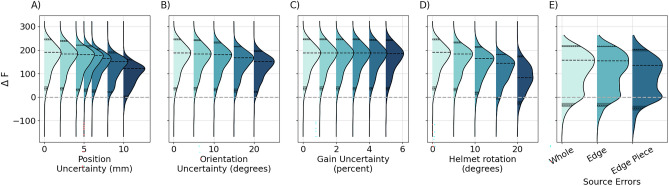
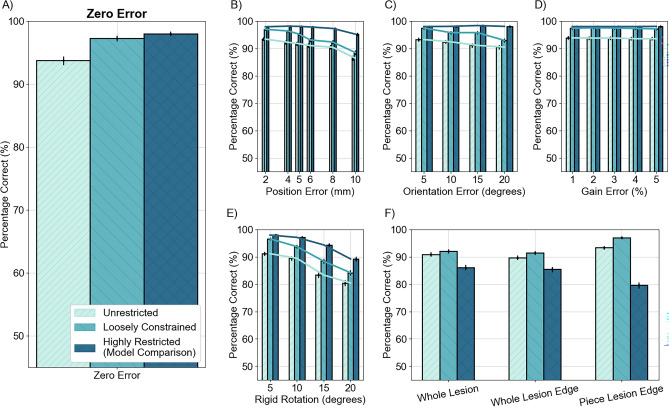
When planning for epilepsy surgery, multiple potential sites for resection may be identified through anatomical imaging. Magnetoencephalography (MEG) using optically pumped sensors (OP-MEG) is a non-invasive functional neuroimaging technique which could be used to help identify the epileptogenic zone from these candidate regions. Here we test the utility of a-priori information from anatomical imaging for differentiating potential lesion sites with OP-MEG. We investigate a number of scenarios: whether to use rigid or flexible sensor arrays, with or without a-priori source information and with or without source modelling errors. We simulated OP-MEG recordings for 1309 potential lesion sites identified from anatomical images in the Multi-centre Epilepsy Lesion Detection (MELD) project. To localise the simulated data, we used three source inversion schemes: unconstrained, prior source locations at centre of the candidate sites, and prior source locations within a volume around the lesion location. We found that prior knowledge of the candidate lesion zones made the inversion robust to errors in sensor gain, orientation and even location. When the reconstruction was too highly restricted and the source assumptions were inaccurate, the utility of this a-priori information was undermined. Overall, we found that constraining the reconstruction to the region including and around the participant's potential lesion sites provided the best compromise of robustness against modelling or measurement error.
© 2024. The Author(s).
Conflict of interest statement
M.J.B. is a director and chairman of, and holds founding equity in Cerca Magnetics Limited, a spin-out company whose aim is to commercialise aspects of OPM-MEG technology. This work was partly funded by a Wellcome award which involves a collaboration agreement with QuSpin, a commercial entity selling optically pumped magnetometers (OPMs).
Figures

References
-
- Engel J, et al. Practice parameter: Temporal lobe and localized neocortical resections for epilepsy: Report of the Quality Standards Subcommittee of the American Academy of Neurology, in Association with the American Epilepsy Society and the American Association of Neurological Surgeons. Neurology. 2003;60:538–547. doi: 10.1212/01.WNL.0000055086.35806.2D. - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
