

Arthroscopic superior capsule reconstruction augmentation using a semitendinosus autograft in massive reparable rotator cuff tears
- PMID: 38312265
- PMCID: PMC10837716
- DOI: 10.1016/j.jseint.2023.08.020
Arthroscopic superior capsule reconstruction augmentation using a semitendinosus autograft in massive reparable rotator cuff tears
Abstract
Background: Arthroscopic superior capsule reconstruction (SCR) augmentation is a viable treatment option for massive reparable cuff tears. This study aimed to retrospectively compare clinical and imaging outcomes of patients with reparable massive rotator cuff tears after arthroscopic rotator cuff repair (ARCR) with those after SCR augmentation using a semitendinosus autograft.
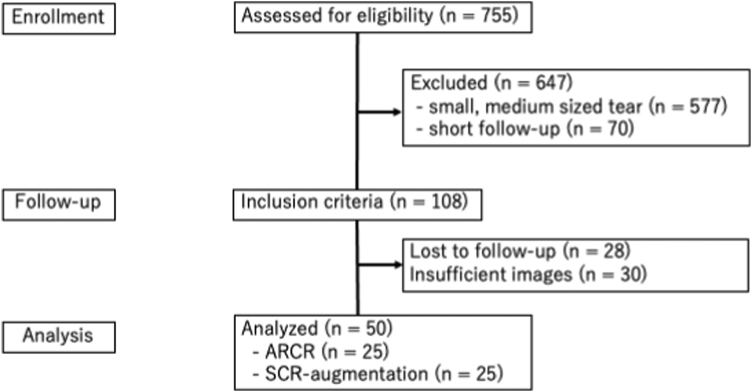
Methods: We retrospectively compared 50 patients with massive reparable rotator cuff tears who underwent ARCR and SCR augmentation (n = 25 each). Patients were clinically followed up for at least 2 years, and the American Shoulder and Elbow index, other patient-reported outcomes, active range of motion, and radiography and magnetic resonance imaging findings were assessed.
Results: At the final follow-up, both patient groups showed significant improvements in forward elevation in range of motion and visual analog scale scores. Improvements in the American Shoulder and Elbow scores in the SCR augmentation group were significantly superior to those in the ARCR group (48.3 and 28.9, P < .01). There was a significant difference in the retear rate between the SCR augmentation group and ARCR group (20% and 56%, respectively; P = .009).
Conclusion: Our study demonstrated that patient-reported outcomes and retear rates in patients who underwent SCR augmentation with rotator cuff repair for massive rotator cuff tears significantly improved compared with those in patients who underwent ARCR without augmentation. Augmentation with semitendinosus autografting during rotator cuff repair represents a solution for patients with massive reparable rotator cuff tears.
Keywords: Augmentation; Rotator cuff; Rotator cuff repair; Semitendinosus tendon; Shoulder; Superior capsule reconstruction.
© 2023 The Author(s).
Figures
Similar articles
-
Superior Capsule Reconstruction for Reinforcement of Arthroscopic Rotator Cuff Repair Improves Cuff Integrity.Am J Sports Med. 2019 Feb;47(2):379-388. doi: 10.1177/0363546518816689. Epub 2018 Dec 31. Am J Sports Med. 2019. PMID: 30596519
-
A meta-analysis of the outcomes of large to massive rotator cuff tears treated with direct repair, graft augmentation, or superior capsular reconstruction.Eur J Orthop Surg Traumatol. 2025 Aug 20;35(1):354. doi: 10.1007/s00590-025-04488-x. Eur J Orthop Surg Traumatol. 2025. PMID: 40836122 Review.
-
Modified Superior Capsule Reconstruction Using the Long Head of the Biceps Tendon as Reinforcement to Rotator Cuff Repair Lowers Retear Rate in Large to Massive Reparable Rotator Cuff Tears.Arthroscopy. 2021 Aug;37(8):2420-2431. doi: 10.1016/j.arthro.2021.04.003. Epub 2021 Apr 15. Arthroscopy. 2021. PMID: 33864834
-
Partial Superior Capsular Reconstruction to Augment Arthroscopic Repair of Massive Rotator Cuff Tears Using Autogenous Biceps Tendon: Effect on Retear Rate.Am J Sports Med. 2022 Sep;50(11):3064-3072. doi: 10.1177/03635465221112659. Epub 2022 Aug 19. Am J Sports Med. 2022. PMID: 35983981
-
A Systematic Review of Long-term Clinical and Radiological Outcomes of Arthroscopic and Open/Mini-open Rotator Cuff Repairs.Am J Sports Med. 2023 Jun;51(7):1904-1913. doi: 10.1177/03635465211073332. Epub 2022 Feb 18. Am J Sports Med. 2023. PMID: 35179393
Cited by
-
A Narrative Review on the Double Pulley-Triple Row Technique for Large to Massive Rotator Cuff Repair.Clin Orthop Surg. 2025 Jun;17(3):359-371. doi: 10.4055/cios24424. Epub 2025 May 15. Clin Orthop Surg. 2025. PMID: 40454127 Free PMC article. Review.
-
Arthroscopic Superior Capsular Reconstruction With Knotless Double-Row Dermal Allograft and Margin Convergence Augmentation.Video J Sports Med. 2025 May 15;5(3):26350254241299461. doi: 10.1177/26350254241299461. eCollection 2025 May-Jun. Video J Sports Med. 2025. PMID: 40386249 Free PMC article.
-
Arthroscopic Superior Capsular Reconstruction Using Autogenous Peroneus Longus Tendon Bridging Repair for Irreparable Rotator Cuff Tear.Arthrosc Tech. 2025 Feb 25;14(6):103477. doi: 10.1016/j.eats.2025.103477. eCollection 2025 Jun. Arthrosc Tech. 2025. PMID: 40656734 Free PMC article.
References
-
- Barth J., Olmos M.I., Swan J., Barthelemy R., Delsol P., Boutsiadis A. Superior capsular reconstruction with the long head of the biceps autograft prevents infraspinatus retear in massive posterosuperior retracted rotator cuff tears. Am J Sports Med. 2020;48:1430–1438. doi: 10.1177/0363546520912220. - DOI - PubMed
-
- Berthold D.P., Bell R., Muench L.N., Jimenez A.E., Cote M.P., Obopilwe E., et al. A new approach to superior capsular reconstruction with hamstring allograft for irreparable posterosuperior rotator cuff tears: a dynamic biomechanical evaluation. J Shoulder Elbow Surg. 2021;30:S38–S47. doi: 10.1016/j.jse.2021.04.002. - DOI - PubMed
-
- Bi M., Ding W., Zheng M., Peng Z., Li J., Ding S. Arthroscopic superior capsule reconstruction with combined fascia lata autograft and synthetic scaffold patch graft for the treatment of irreparable rotator cuff tears yields favorable clinical and radiographic outcomes at minimum two-year follow-up. Arthroscopy. 2023;39:1800–1810. doi: 10.1016/j.arthro.2023.02.025. - DOI - PubMed
-
- Burkhart S.S. Reconciling the paradox of rotator cuff repair versus debridement: a unified biomechanical rationale for the treatment of rotator cuff tears. Arthroscopy. 1994;10:4–19. - PubMed
LinkOut - more resources
Full Text Sources