

doi: 10.1016/j.eats.2023.09.003.
eCollection 2024 Jan.
Arthroscopic Posterior Glenoid Osteotomy
Affiliations
- PMID: 38312878
- PMCID: PMC10837975
- DOI: 10.1016/j.eats.2023.09.003
Item in Clipboard
Arthroscopic Posterior Glenoid Osteotomy
Arthrosc Tech.
.
Abstract
Management of posterior shoulder instability in patients with excessive glenoid retroversion can be challenging. However, a corrective posterior glenoid osteotomy is an option. Although various open techniques are available, minimally invasive and arthroscopy surgery are the most advantageous. This study describes the feasibility and safety of an arthroscopic posterior open wedge glenoid osteotomy using an autologous scapular spine graft along with additional posterior capsulolabral complex reattachment. This procedure is a viable option for patients with symptomatic posterior shoulder instability.
© 2023 The Authors.
Figures

Right shoulder, lateral decubitus position, external view. (A) Arthroscopic scope was inserted through the anterosuperolateral portal, Shaver handpiece through the posterior standard portal, and the blue cannula (C) through the anterior rotator interval portal. (B) The dotted marks indicate the horizontal approach over the midpoint of the scapula spine for bone autograft harvesting. (C) Triangular-shaped tricortical bone scapular spine autograft. (D) The dorsal view of the right scapula depicts the specific area from where the graft is harvested. (A, anterior portal; AS, anterosuperolateral portal; C, cannula; P, posterior portal; S, Shaver handpiece; V, lateral vertical strap.)

Right shoulder, lateral decubitus position. (A) Extra-articular view shows the routine portals: posterior, anterior, anterosuperolateral (ASL), and an accessory posteroinferior portal. A switching stick is inserted through the standard posterior portal. (B, C) Arthroscopic view from the ASL portal. Notice the complete detachment of the posterior capsulolabral complex and thorough debridement of the posterior glenoid rim and wall. (D) The needle is introduced to establish the appropriate level for the posteroinferior working osteotomy portal. The dotted line marks the scapula spine approach. (A, anterior portal; AS, anterosuperolateral portal; C, capsulolabral complex; G, glenoid; H, humerus; P, posterior portal; Pi, posteroinferior portal.)

Right shoulder, lateral decubitus position. (A) Extra-articular view. The open metallic cannula is introduced underneath the switching stick through the accessory posteroinferior portal. (B, C) Arthroscopic view from the AS portal depicts the switching stick and the open metallic cannula. (D) The rod is exchanged with the drill guide hook. The dotted line marks the scapula spine approach. (AS, anterosuperolateral portal; G, glenoid; H, humerus; Ho, drill guide hook; P, posterior portal; Pi, posteroinferior portal; OC, open metallic cannula; SS, switching stick.)

Right shoulder, lateral decubitus position. (A, B) Arthroscopic view. The drill guide sleeve assembled to the handle of the drill guide hook is introduced from the posteroinferior working portal. (C) Schematic representation illustrates the specific hook and drill guide. (DG, drill guide; G, glenoid; H, humerus; Ho, drill guide hook.)

Right shoulder, lateral decubitus position. Drill 2 k-wires through the specific drill guide. (A, B) Drill hook is introduced from the posteroinferior working portal. (C) External view. (D) Schematic representation; the k-wires through the specific drill guide stop short of breaking through the anterior cortex. The dotted line marks the scapula spine approach. (AS, arthroscopy scope; G, glenoid; H, humerus; DG, specific drill guide; Ho, drill guide hook.)

Right shoulder, lateral decubitus position. (A, B) Anterosuperolateral scope view. The k-wires are exposed, and the forked retractor is posteriorly introduced. (C) External view. A forked retractor with rails is inserted beneath the k-wires. (D) The osteotome is introduced over the retractor and in between the k-wires, impacting into the bone. (E) Schematic representation. Notice the osteotome under the k-wires. (C, capsulolabral complex; G, glenoid; H, humerus; K, k-wires; O, osteotome; R, forked retractor.)

Right shoulder, lateral decubitus position. Change the orientation of the cut inferiorly and superiorly to complete the osteotomy. Posterior external view: (A) inferior orientation and (B) superior orientation. Arthroscopic view: (C) notice the osteotome with inferior and (D) with superior direction. The dotted line marks the scapula spine approach. (O, osteotome; P, posterior portal; Pi, posteroinferior portal; R, forked retractor.)

Right shoulder, lateral decubitus position. (A) Arthroscopic view. The forked retractor and the blunt retractor are introduced together into the posterior osteotomy. (B) External view. The forked and blunt retractors open the osteotomy wedge. (C) Schematic representation. The dotted line marks the scapula spine approach. (B, blunt retractor; G, glenoid; H, humerus; P, posterior portal; P, posterior portal; Pi, posteroinferior portal; R, forked retractor.)
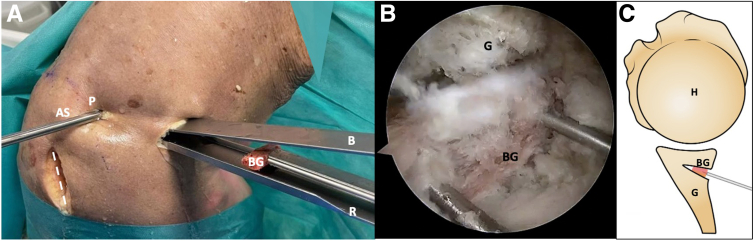
Right shoulder, lateral decubitus position. (A) The scapular spine autograft is introduced using 2 small k-wires, and then is slides over the retractor. (B) Arthroscopic view from the posterolateral portal. The graft is positioned using k-wires. (C) Schematic representation in axial view. The dotted line marks the scapula spine approach. (AS, arthroscopy scope; B, blunt retractor; BG, bone graft; G, glenoid; H, humerus; P, posterior portal; R, retractor.)

Right shoulder, lateral decubitus position. (A) Anterosuperolateral scope view portal. To reattach the capsulolabral complex to the posterior glenoid rim, 2 or 3 soft anchor implants are required to pass through the graft and reach the medial body of the scapula. (B) Posterior external view. Notice that 2 soft anchors have been inserted through the posteroinferior working portal. (C) Schematic representation. Axial view of the final procedure showing the use of an anchor for stabilizing both the osteotomy and graft. The dotted line marks the scapula spine approach. (BG, bone graft; C, capsulolabral complex; G, glenoid; H, humerus; P, posterior portal; Pi, posteroinferior portal.)

Schematic representation: the arthroscopic posterior glenoid osteotomy summary. (A) The specific drill guide is introduced through the posteroinferior working portal to drill 2 k-wires. (B) A forked retractor and osteotome are positioned between the k-wires. (C) The blunt retractor is positioned above the forked retractor to create and open the osteotomy. (D) The triangular scapular spine autograft is inserted and impacted while maintaining the open wedge osteotomy. (E) The capsulolabral complex is reattached to the posterior glenoid rim using implants that pass through the graft and reach the medial body of the scapula. (F) Final sagittal view. (B, blunt retractor; BG,bone graft; G, glenoid; H, humerus; Ho, drill guide hook; DG, specific drill guide; O, osteotome; R, forked retractor.)
References
-
- Robinson C.M., Seah M., Akhtar M.A. The epidemiology, risk of recurrence, and functional outcome after an acute traumatic posterior dislocation of the shoulder. J Bone Joint Surg. 2011;93:1605–1613. - PubMed
-
- Provencher M.T., Bhatia S., Ghodadra N.S., et al. Recurrent shoulder instability: Current concepts for evaluation and management of glenoid bone loss. J Bone Joint Surg. 2010;92:133–151. (suppl 2) - PubMed
-
- Malik S.S., Jordan R.W., Tahir M., MacDonald P.B. Does the posterior glenoid osteotomy reduce the rate of recurrence in patients with posterior shoulder instability: A systematic review. Orthop Traumatol Surg Res. 2021;107:102760. - PubMed
