

Relationship Between Diet Quality and Antihypertensive Medication Intensity Among Adults With Metabolic Syndrome-Associated High Blood Pressure
- PMID: 38313343
- PMCID: PMC10837706
- DOI: 10.1016/j.cjco.2023.09.016
Relationship Between Diet Quality and Antihypertensive Medication Intensity Among Adults With Metabolic Syndrome-Associated High Blood Pressure
Abstract
Background: Management of high blood pressure (BP), a key feature of the metabolic syndrome (MetS), relies on diet and medication. Whether these modalities are used as complements has never been evaluated in real-world settings. This study assessed the relationship between diet quality and antihypertensive medication intensity among adults with MetS-associated high BP.
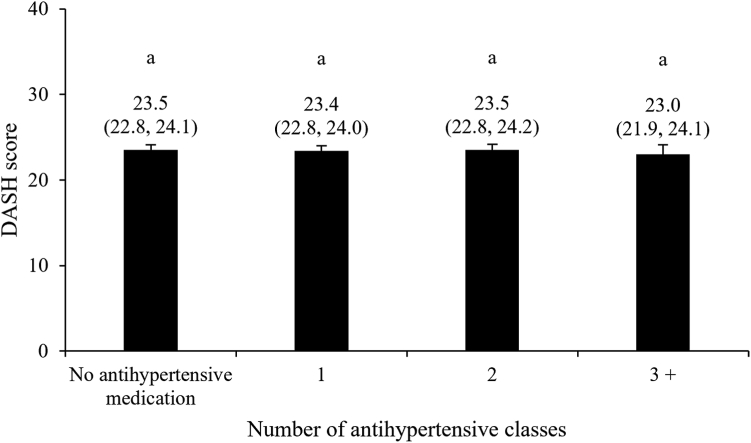
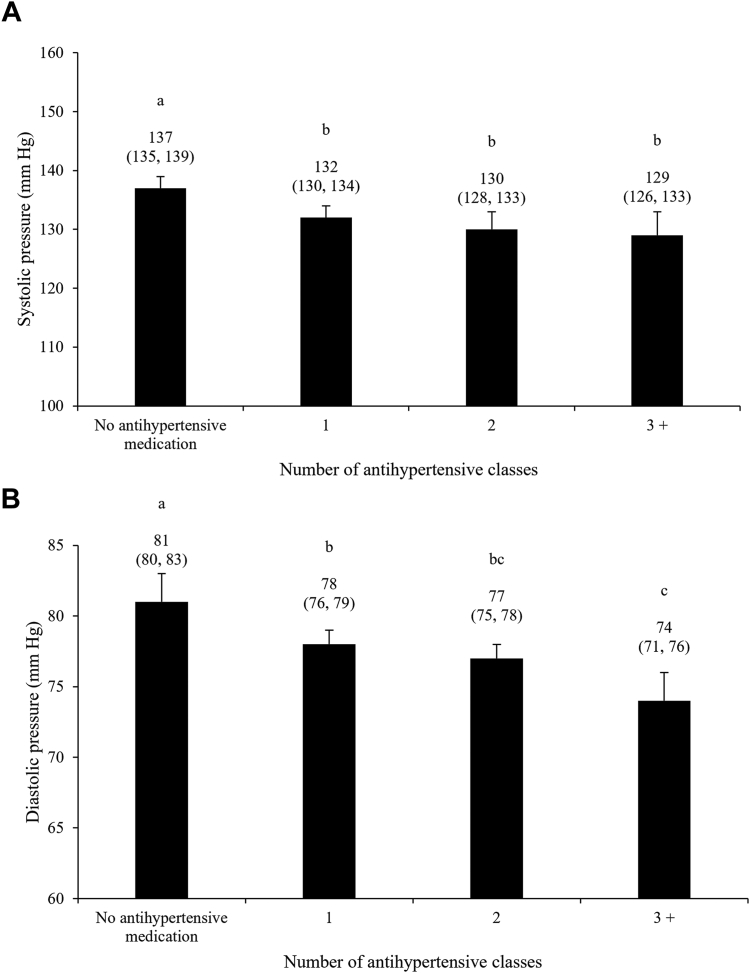
Methods: This cross-sectional study included 915 adults with MetS-associated high BP from the CARTaGENE cohort (Québec, Canada), of whom 677 reported using BP-lowering medication. Antihypertensive medication intensity was graded per the number of BP-lowering classes used simultaneously. Diet quality was assessed using the Dietary Approach to Stop Hypertension (DASH) score.
Results: No evidence of a relationship between antihypertensive medication intensity and diet quality was found (β for each additional antihypertensive = -0.05; 95% CI, -0.35; 0.26 DASH score points). However, among men aged < 50 years and women aged < 60 years, the DASH score was inversely associated with medication intensity (β = -0.72; 95% CI, -1.24, -0.19), whereas this relationship tended to be positive among older participants (β = 0.32; 95% CI, -0.05, 0.69). Among participants with low Framingham risk score, the DASH score was inversely associated with medication intensity (β = -0.70; 95% CI, -1.31, -0.09), but no evidence of an association was found among individuals at moderate (β = 0.00; 95% CI, -0.45, 0.45) or high (β = 0.30, 95% CI, -0.24, 0.84) risk.
Conclusions: In this cohort of adults with MetS-associated high BP, there was an overall lack of complementarity between diet quality and BP-lowering medication, especially among younger individuals and those with a lower risk for cardiovascular disease for whom diet quality was inversely associated with intensity of medication.
Introduction: La prise en charge de la pression artérielle (PA) élevée, l’une des caractéristiques principales du syndrome métabolique (SMet), repose sur une saine alimentation et l'usage de médicaments hypotenseurs. Il n’a jamais été évalué si ces modalités étaient utilisées de façon complémentaire en contexte réel. La présente étude portait sur la relation entre la qualité de l'alimentation et la médication antihypertensive au sein d'adultes ayant une PA élevée associée au SMet.
Méthodes: Cette étude transversale regroupait 915 adultes de la cohorte CARTaGENE (Québec, Canada) ayant une PA élevée associée au SMet, dont 677 ont rapporté prendre des médicaments abaissant la PA. L’intensité de la médication antihypertensive a été évaluée par le nombre de classes de médicaments abaissant la PA utilisées simultanément. La qualité du régime alimentaire a été évaluée à l’aide du score Dietary Approache to Stop Hypertension (DASH).
Résultats: Aucune évidence d’une relation entre l’intensité des médicaments antihypertenseurs et la qualité de l'alimentation n’a été observée (β pour chaque antihypertenseur supplémentaire = –0,05 ; intervalle de confiance [IC] à 95 %, –0,35 ; 0,26 point au score DASH). Toutefois, chez les hommes âgés < 50 ans et chez les femmes âgées < 60 ans, le score DASH était inversement associé à l’intensité des médicaments (β = –0,72 ; IC à 95 %, –1,24, –0,19), alors que cette relation avait tendance à être positive chez les participants plus âgés (β = 0,32 ; IC à 95 %, –0,05, 0,69). Chez les participants qui avaient un score de risque de Framingham faible, le score DASH était inversement associé à l’intensité des médicaments (β = –0,70 ; IC à 95 %, –1,31, –0,09), mais aucune évidence d’une association n’a été observée chez les individus qui avaient un risque modéré (β = 0,00 ; IC à 95 %, –0,45, 0,45) ou élevé (β = 0,30, IC à 95 %, –0,24, 0,84).
Conclusions: Au sein de cette cohorte d’adultes qui avaient une PA élevée associée au SMet, aucune évidence de complémentarité entre la qualité de l'alimentation et l'intensité de la médication antihypertensive n'a été observée, particulièrement chez les individus plus jeunes et chez ceux exposés à un risque plus faible de maladies cardiovasculaires pour qui la qualité du régime alimentaire était inversement associée à l’intensité des médicaments.
© 2023 The Authors.
Figures
Similar articles
-
Relationship Between Diet Quality and Glucose-Lowering Medication Intensity Among Adults With Type 2 Diabetes: Results From the CARTaGENE Cohort.CJC Open. 2023 Sep 29;6(1):20-29. doi: 10.1016/j.cjco.2023.09.015. eCollection 2024 Jan. CJC Open. 2023. PMID: 38313340 Free PMC article.
-
Relationship Between Diet Quality and Statin Use Among Adults With Metabolic Syndrome From the CARTaGENE Cohort.CJC Open. 2023 Sep 29;6(1):11-19. doi: 10.1016/j.cjco.2023.09.014. eCollection 2024 Jan. CJC Open. 2023. PMID: 38313338 Free PMC article.
-
Higher Diet Quality in African-American Adolescents Is Associated with Lower Odds of Metabolic Syndrome: Evidence from the NHANES.J Nutr. 2021 Jun 1;151(6):1609-1617. doi: 10.1093/jn/nxab027. J Nutr. 2021. PMID: 33768240 Free PMC article.
-
The Use of Dietary Approaches to Stop Hypertension (DASH) Mobile Apps for Supporting a Healthy Diet and Controlling Hypertension in Adults: Systematic Review.JMIR Cardio. 2022 Nov 2;6(2):e35876. doi: 10.2196/35876. JMIR Cardio. 2022. PMID: 36322108 Free PMC article. Review.
-
Overview of salt restriction in the Dietary Approaches to Stop Hypertension (DASH) and the Mediterranean diet for blood pressure reduction.Rev Cardiovasc Med. 2022 Jan 19;23(1):36. doi: 10.31083/j.rcm2301036. Rev Cardiovasc Med. 2022. PMID: 35092228 Review.
Cited by
-
Multidisciplinary Care in a Public University Family Medicine Group in Québec (Canada): Data on Patients' Follow-Up and Cardiometabolic Risk Management.Healthcare (Basel). 2025 Jul 15;13(14):1704. doi: 10.3390/healthcare13141704. Healthcare (Basel). 2025. PMID: 40724729 Free PMC article.
-
Gender differences in the association between adherence to healthy diet principles and adherence to cardiopreventive medication among adults from Québec (Canada).Br J Nutr. 2025 Jan 16;133(3):1-11. doi: 10.1017/S0007114525000030. Online ahead of print. Br J Nutr. 2025. PMID: 39817436 Free PMC article.
-
Cohort profile: the CARTaGENE Cohort Nutrition Study (Quebec, Canada).BMJ Open. 2024 Aug 17;14(8):e083425. doi: 10.1136/bmjopen-2023-083425. BMJ Open. 2024. PMID: 39153764 Free PMC article.
References
-
- Després J.P. Is visceral obesity the cause of the metabolic syndrome? Ann Med. 2006;38:52–63. - PubMed
-
- Rao D.P., Dai S., Lagacé C., Krewski D. Metabolic syndrome and chronic disease. Chronic Dis Inj Can. 2014;34:36–45. - PubMed
-
- Katsimardou A., Imprialos K., Stavropoulos K., Sachinidis A., Doumas M., Athyros V. Hypertension in metabolic syndrome: novel insights. Curr Hypertens Rev. 2020;16:12–18. - PubMed
-
- Barrios V., Escobar C., Calderon A., et al. Prevalence of the metabolic syndrome in patients with hypertension treated in general practice in Spain: an assessment of blood pressure and low-density lipoprotein cholesterol control and accuracy of diagnosis. J Cardiometab Syndr. 2007;2:9–15. - PubMed
LinkOut - more resources
Full Text Sources
