

Open Dislocation of the Scaphoid With an Associated Hamate Fracture and Fourth Metacarpal Fracture
- PMID: 38313608
- PMCID: PMC10837301
- DOI: 10.1016/j.jhsg.2023.10.004
Open Dislocation of the Scaphoid With an Associated Hamate Fracture and Fourth Metacarpal Fracture
Abstract
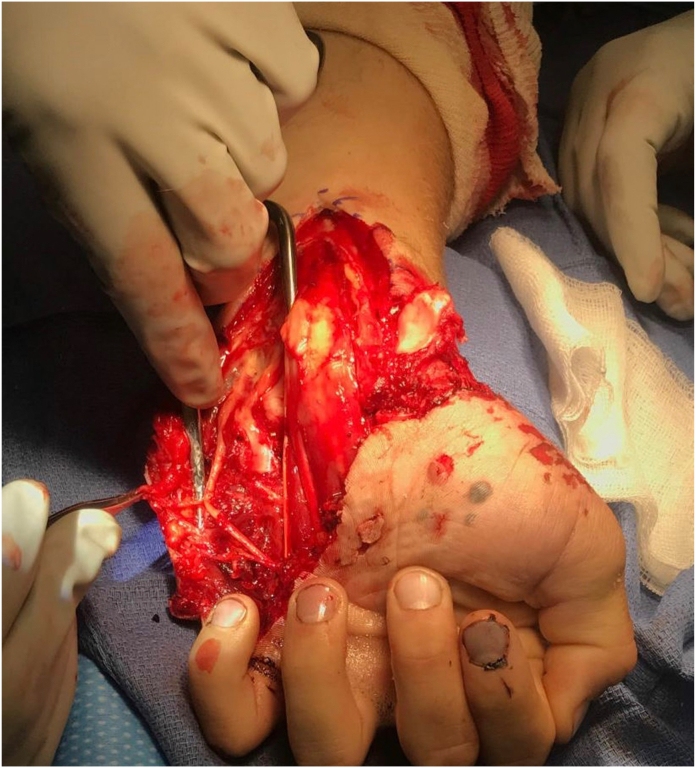
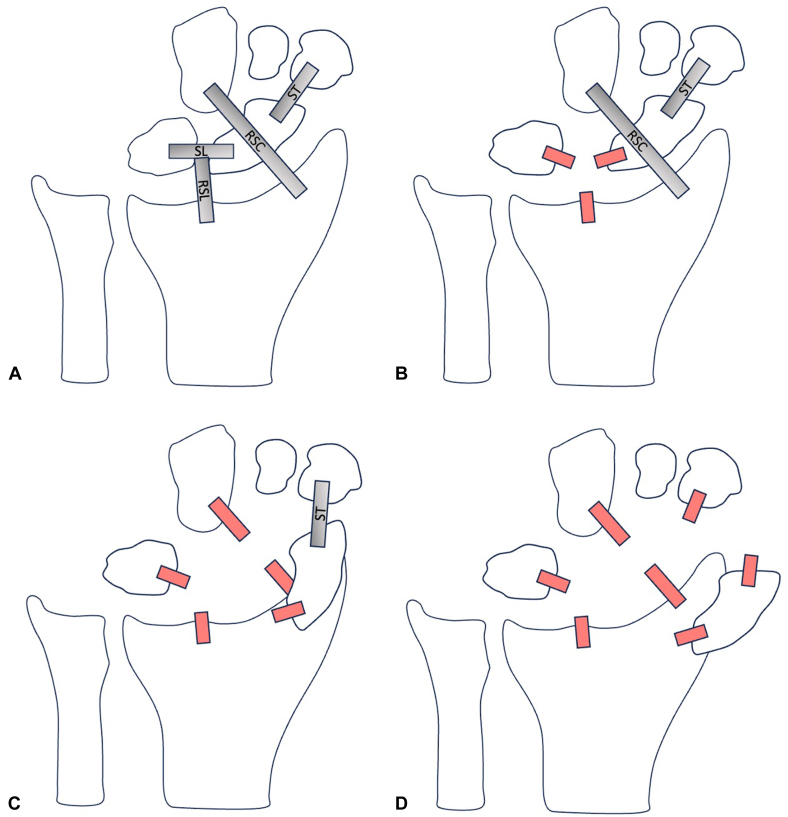
Scaphoid dislocation represents a rare injury with only a few case reports and limited case series reported in the literature. The majority of scaphoid dislocations result from a high-energy trauma causing hyperextension and ulnar deviation of the wrist. The severity of a scaphoid dislocation depends on the degree of periscaphoid ligamentous injury as well as the presence of concomitant injuries, such as axial carpal dissociation. The most common complication after a scaphoid dislocation is scapholunate dissociation, which emphasizes the importance of scapholunate ligament repair/reconstruction in these cases. We report a case of an open scaphoid dislocation with the associated injuries of a hamate fracture and fourth metacarpal fracture treated with an open reduction of the scaphoid, open ligamentous repair and augmentation of the involved carpal ligaments, and open reduction internal fixation of both the hamate and the fourth metacarpal fractures.
Keywords: Fourth metacarpal fracture; Hamate fracture; Open; Scaphoid dislocation; Volar.
© 2023 The Authors.
Figures






References
-
- Chloros G.D., Themistocleous G.S., Zagoreos N.P., et al. Isolated dislocation of the scaphoid. Arch Orthop Trauma Surg. 2006;126(3):197–203. - PubMed
-
- Amamilo S.C., Uppal R., Samuel A.W. Isolated dislocation of carpal scaphoid. J Hand Surg Br. 1985;10(3):385–388. - PubMed
-
- Thompson T.C., Campbell R.D., Arnold W.D. Primary and secondary dislocation of the scaphoid bone. J Bone Joint Surg Br. 1964;46(1):73–82. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
