

Vulnerabilities and reparative strategies during pregnancy, childbirth, and the postpartum period: moving from rhetoric to action
- PMID: 38314056
- PMCID: PMC10837549
- DOI: 10.1016/j.eclinm.2023.102264
Vulnerabilities and reparative strategies during pregnancy, childbirth, and the postpartum period: moving from rhetoric to action
Abstract
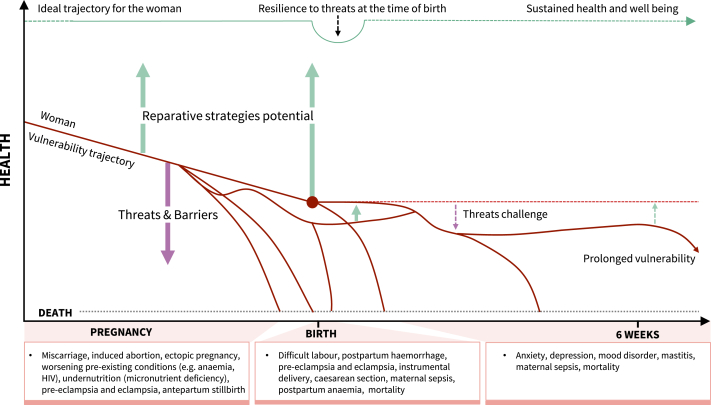
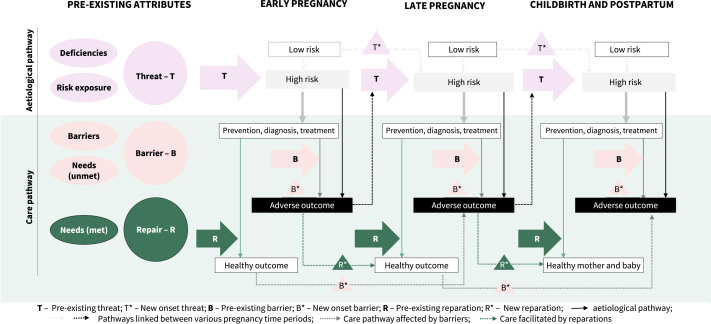
Maternal outcomes throughout pregnancy, childbirth, and the postnatal period are influenced by interlinked and interdependent vulnerabilities. A comprehensive understanding of how various threats and barriers affect maternal and perinatal health is critical to plan, evaluate and improve maternal health programmes. This paper builds on the introductory paper of the Series on the determinants of maternal health by assessing vulnerabilities during pregnancy, childbirth, and the postnatal period. We synthesise and present the concept of vulnerability in pregnancy and childbirth, and map vulnerability attributes and their dynamic influence on maternal outcomes in early and late pregnancy and during childbirth and the postnatal period, with a particular focus on low-income and middle-income countries (LMICs). We summarise existing literature and present the evidence on the effects of various reparative strategies to improve pregnancy and childbirth outcomes. Lastly, we discuss the implications of the identified vulnerability attributes and reparative strategies for the efforts of policymakers, healthcare professionals, and researchers working towards improving outcomes for women and birthing people in LMICs.
Keywords: LMIC; Pregnant; Vulnerability.
© 2023 World Health Organization.
Conflict of interest statement
All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work. The contents of the paper are the sole responsibility of the authors and do not necessarily represent the official views, decisions, or policies of HRP, World Health Organization or other authors’ organisations.
Figures
Comment in
-
Maternal health in a dramatically different world: tailoring actions to achieve targets for 2030 and beyond.Lancet Glob Health. 2024 Feb;12(2):e185-e187. doi: 10.1016/S2214-109X(23)00545-4. Epub 2023 Dec 6. Lancet Glob Health. 2024. PMID: 38070537 No abstract available.
References
-
- Scheele J., Harmsen van der Vliet–Torij H.W., Wingelaar-Loomans E.M., Goumans M.J.B.M. Defining vulnerability in European pregnant women, a Delphi study. Midwifery. 2020;86 - PubMed
-
- World Health Organization . World Health Organization; Geneva: 2019. Trends in maternal mortality 2000 to 2017: estimates by WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division.https://apps.who.int/iris/handle/10665/327595 [accessed 2022 Nov 6]. Available from:
-
- Waisel D.B. Vulnerable populations in healthcare. Curr Opin Anesthesiol. 2013;26(2):186. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
