

Effects of inpatient creatinine testing frequency on acute kidney injury identification and staging: a historical cohort study
- PMID: 38315304
- PMCID: PMC11133048
- DOI: 10.1007/s11096-023-01697-4
Effects of inpatient creatinine testing frequency on acute kidney injury identification and staging: a historical cohort study
Abstract
Background: Acute kidney injury (AKI) is a multifactorial condition often induced by drugs commonly used in hospitals. Identifying and staging AKI necessitates frequent monitoring of renal function.
Aim: To assess the impact of real-world hospital practices regarding serum creatinine (SCr) testing on the identification and staging of AKI, and its implications for adjusting drug doses.
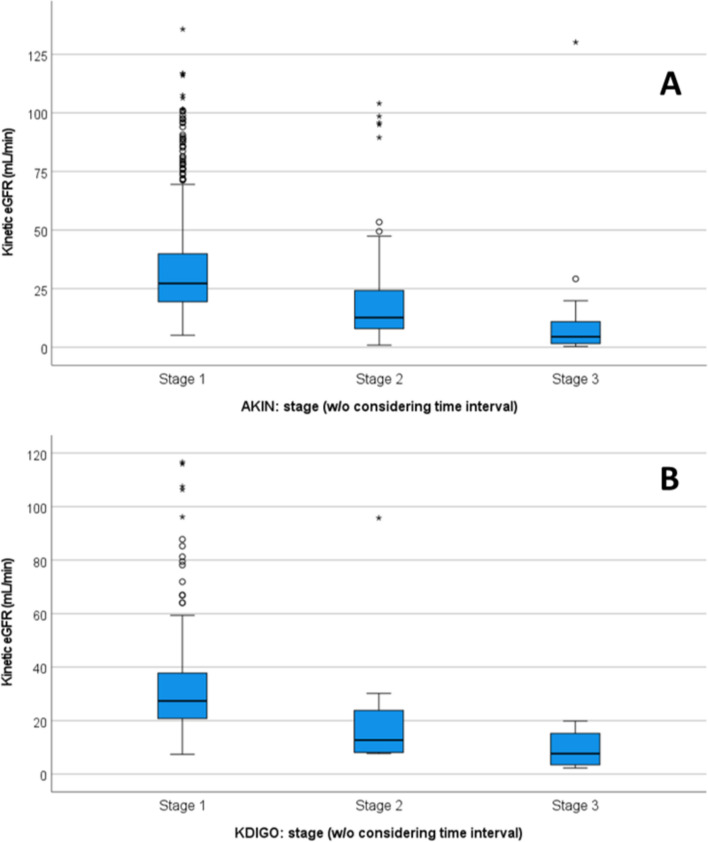
Method: A historical cohort study utilizing hospital records from all adult patients admitted between 01/06/2018 and 31/12/2020 was conducted. Patients with no SCr assessment during their stay or those with an SCr at admission ≥ 2 mg/dL were excluded. AKI was determined using two criteria, namely AKIN and KDIGO, considering the time intervals between two SCr tests as outlined in the criteria. Additionally, patients with SCr increases exceeding AKI limits, regardless the time interval, were also identified. The estimated glomerular filtration rate (eGFR) and kinetic eGFR (KeGFR) were calculated.
Results: During the study period, 17,269 hospitalizations and 62,255 SCr tests were recorded. Among the 17,032 hospitalizations with a length of stay > 48 h, 46.8% experienced periods with no SCr tests performed for more than 48 h. Any stage of AKI was identified in 7.0% of patients and in 9.1% using AKI and KDIGO criteria, respectively. Ignoring time limits in both criteria revealed potential AKI in 1942 patients (11.2%), indicating a potential underdiagnosis of AKI by 37.5% or 19.1%, depending on the criteria used. A total of 76 drugs requiring dose adjustment in patients with eGFR ≤ 50 ml/min were prescribed in 78.5% admissions. These drugs were prescribed in 87.9% of patients potentially underdiagnosed with AKIN and in 88.9% with KDIGO.
Conclusion: There is a need for changes in the established hospital procedures to ensure more frequent testing of SCr levels. Implementing an advanced scope of practice for clinical pharmacists could support these changes.
Keywords: Acute kidney injury; Drug-related side effects and adverse reactions; Hospital; Pharmacoepidemiology; Pharmacy service; Retrospective studies.
© 2024. The Author(s).
Conflict of interest statement
FAC is associate editor of the International Journal of Clinical Pharmacy but was not involved in the review process of this manuscript. The other authors have no conflicts of interest to declare.
Figures
Similar articles
-
Using the Kinetic Estimating Glomerular Filtration Rate Equation for Estimating Glomerular Filtration Rate and Detecting Acute Kidney Injury: A Pilot Study.Nephron. 2018;140(4):231-239. doi: 10.1159/000492439. Epub 2018 Sep 19. Nephron. 2018. PMID: 30231255
-
Comparison of absolute serum creatinine changes versus Kidney Disease: Improving Global Outcomes consensus definitions for characterizing stages of acute kidney injury.Nephrol Dial Transplant. 2013 Jun;28(6):1447-54. doi: 10.1093/ndt/gfs533. Epub 2013 Jan 25. Nephrol Dial Transplant. 2013. PMID: 23355628 Free PMC article.
-
Evaluation of the accuracy of estimated baseline serum creatinine for acute kidney injury diagnosis.Clin Exp Nephrol. 2018 Apr;22(2):405-412. doi: 10.1007/s10157-017-1481-y. Epub 2017 Oct 5. Clin Exp Nephrol. 2018. PMID: 28983757
-
The definitions and staging systems of acute kidney injury and their limitations in practice.Arab J Nephrol Transplant. 2013 Sep;6(3):145-52. Arab J Nephrol Transplant. 2013. PMID: 24053740 Review.
-
Incidence, timing and outcome of AKI in critically ill patients varies with the definition used and the addition of urine output criteria.BMC Nephrol. 2017 Feb 20;18(1):70. doi: 10.1186/s12882-017-0487-8. BMC Nephrol. 2017. PMID: 28219327 Free PMC article. Review.
Cited by
-
A case/non-case study of a national pharmacovigilance database to explore drug-induced acute kidney injury.Int J Clin Pharm. 2025 May 26. doi: 10.1007/s11096-025-01940-0. Online ahead of print. Int J Clin Pharm. 2025. PMID: 40418435
-
Influence of the estimated glomerular filtration rate equation on carboplatin dosing: a real-world study.Front Pharmacol. 2025 Jun 11;16:1605458. doi: 10.3389/fphar.2025.1605458. eCollection 2025. Front Pharmacol. 2025. PMID: 40567373 Free PMC article.
References
-
- Goh CY, Visvanathan R, Leong CT, et al. A prospective study of incidence and outcome of acute kidney injury among hospitalised patients in Malaysia (My-AKI) Med J Malaysia. 2023;78(6):733–742. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
