

Health effects associated with chewing tobacco: a Burden of Proof study
- PMID: 38316758
- PMCID: PMC10844244
- DOI: 10.1038/s41467-024-45074-9
Health effects associated with chewing tobacco: a Burden of Proof study
Abstract
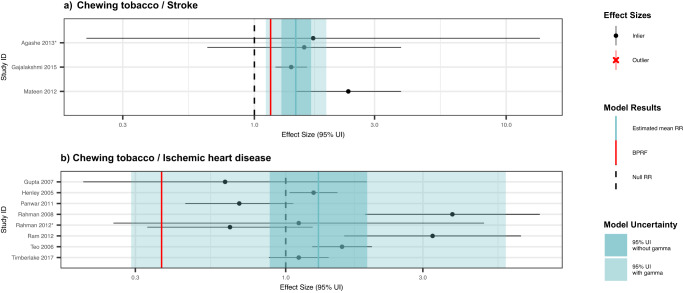
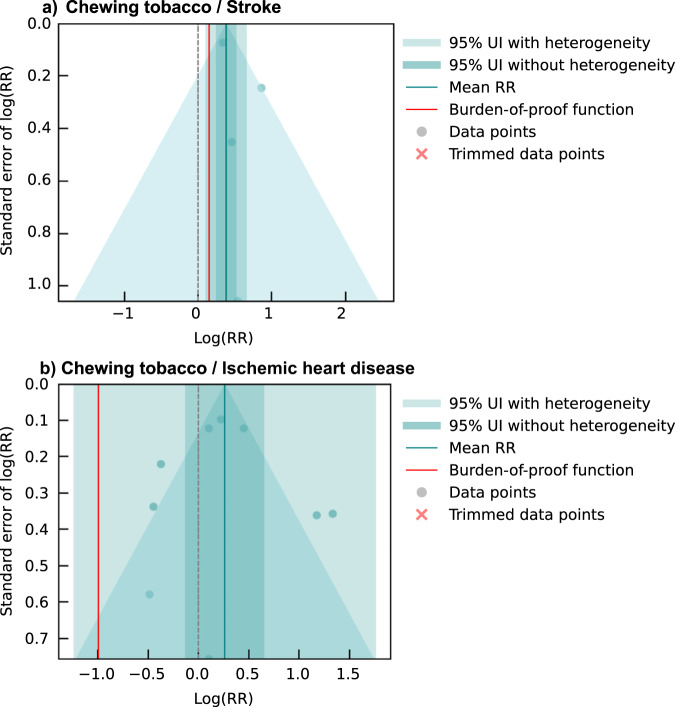
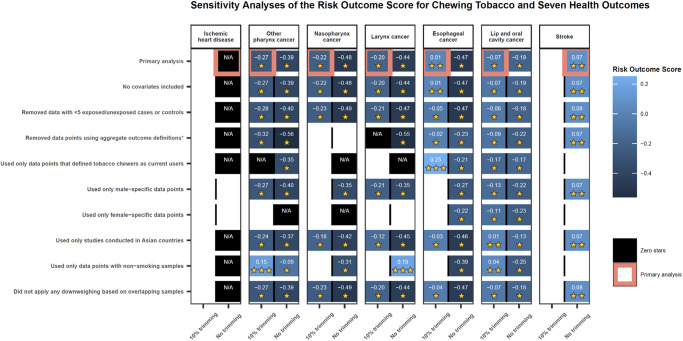
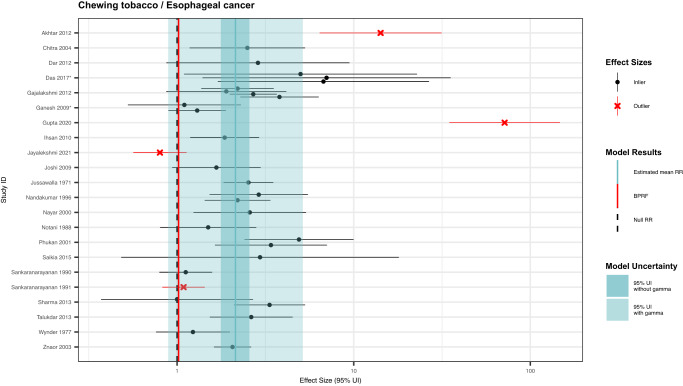
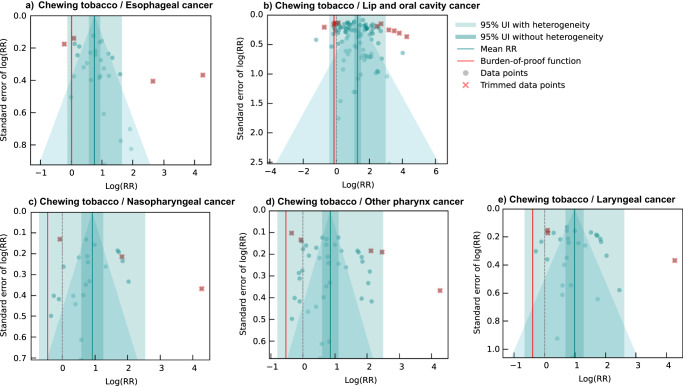
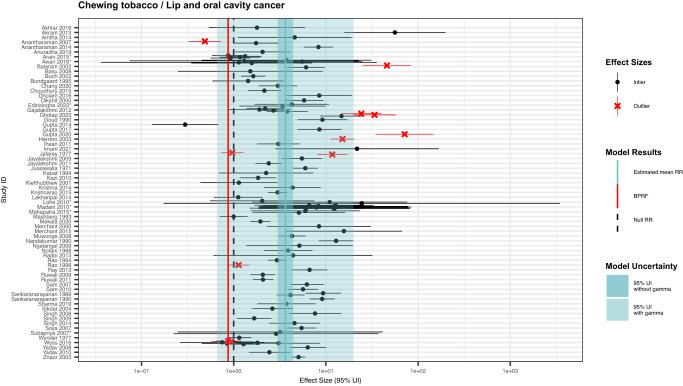
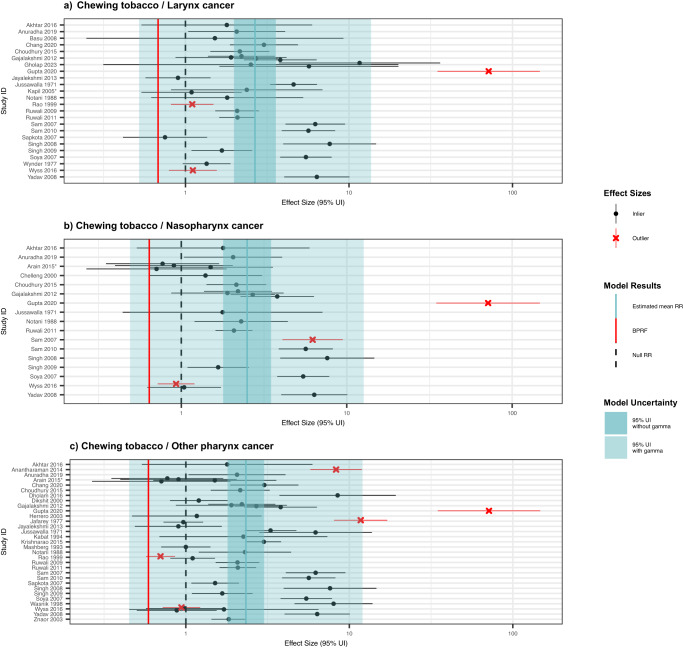
Chewing tobacco use poses serious health risks; yet it has not received as much attention as other tobacco-related products. This study synthesizes existing evidence regarding the health impacts of chewing tobacco while accounting for various sources of uncertainty. We conducted a systematic review and meta-analysis of chewing tobacco and seven health outcomes, drawing on 103 studies published from 1970 to 2023. We use a Burden of Proof meta-analysis to generate conservative risk estimates and find weak-to-moderate evidence that tobacco chewers have an increased risk of stroke, lip and oral cavity cancer, esophageal cancer, nasopharynx cancer, other pharynx cancer, and laryngeal cancer. We additionally find insufficient evidence of an association between chewing tobacco and ischemic heart disease. Our findings highlight a need for policy makers, researchers, and communities at risk to devote greater attention to chewing tobacco by both advancing tobacco control efforts and investing in strengthening the existing evidence base.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Implementation practices in smokeless tobacco control. 28 https://fctc.who.int/publications/i/item/implementation-practices-in-smo... (2022).
-
- WHO FCTC. Smokeless tobacco (SLT) products. WHO Framework Convention on Tobacco Controlhttps://extranet.who.int/fctcapps/fctcapps/fctc/kh/slt/news/smokeless-to... (2018).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
