

The effects of short-term, progressive exercise training on disease activity in smouldering multiple myeloma and monoclonal gammopathy of undetermined significance: a single-arm pilot study
- PMID: 38317104
- PMCID: PMC10840198
- DOI: 10.1186/s12885-024-11817-6
The effects of short-term, progressive exercise training on disease activity in smouldering multiple myeloma and monoclonal gammopathy of undetermined significance: a single-arm pilot study
Abstract
Background: High levels of physical activity are associated with reduced risk of the blood cancer multiple myeloma (MM). MM is preceded by the asymptomatic stages of monoclonal gammopathy of undetermined significance (MGUS) and smouldering multiple myeloma (SMM) which are clinically managed by watchful waiting. A case study (N = 1) of a former elite athlete aged 44 years previously indicated that a multi-modal exercise programme reversed SMM disease activity. To build from this prior case study, the present pilot study firstly examined if short-term exercise training was feasible and safe for a group of MGUS and SMM patients, and secondly investigated the effects on MGUS/SMM disease activity.
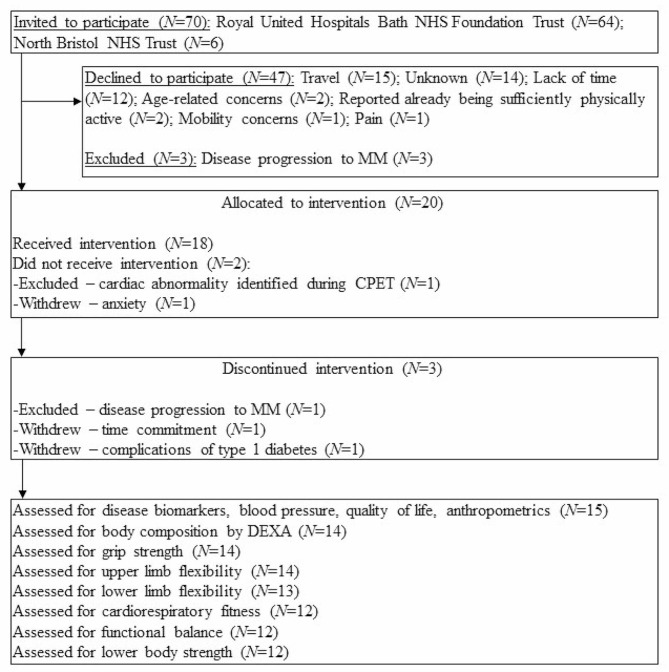
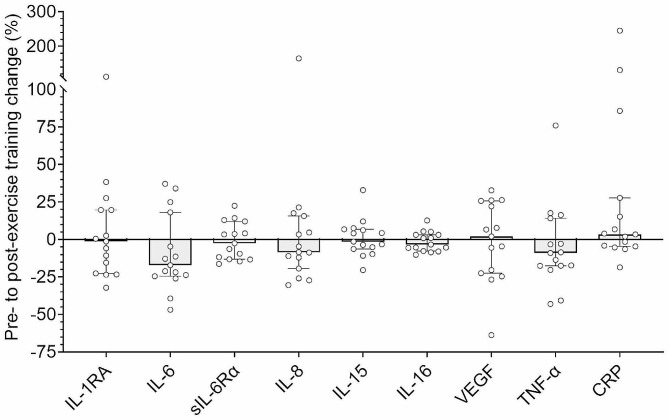
Methods: In this single-arm pilot study, N = 20 participants diagnosed with MGUS or SMM were allocated to receive a 16-week progressive exercise programme. Primary outcome measures were feasibility and safety. Secondary outcomes were pre- to post-exercise training changes to blood biomarkers of MGUS and SMM disease activity- monoclonal (M)-protein and free light chains (FLC)- plus cardiorespiratory and functional fitness, body composition, quality of life, blood immunophenotype, and blood biomarkers of inflammation.
Results: Fifteen (3 MGUS and 12 SMM) participants completed the exercise programme. Adherence was 91 ± 11%. Compliance was 75 ± 25% overall, with a notable decline in compliance at intensities > 70% V̇O2PEAK. There were no serious adverse events. There were no changes to M-protein (0.0 ± 1.0 g/L, P =.903), involved FLC (+ 1.8 ± 16.8 mg/L, P =.839), or FLC difference (+ 0.2 ± 15.6 mg/L, P =.946) from pre- to post-exercise training. There were pre- to post-exercise training improvements to diastolic blood pressure (- 3 ± 5 mmHg, P =.033), sit-to-stand test performance (+ 5 ± 5 repetitions, P =.002), and energy/fatigue scores (+ 10 ± 15%, P =.026). Other secondary outcomes were unchanged.
Conclusions: A 16-week progressive exercise programme was feasible and safe, but did not reverse MGUS/SMM disease activity, contrasting a prior case study showing that five years of exercise training reversed SMM in a 44-year-old former athlete. Longer exercise interventions should be explored in a group of MGUS/SMM patients, with measurements of disease biomarkers, along with rates of disease progression (i.e., MGUS/SMM to MM).
Registration: https://www.isrctn.com/ISRCTN65527208 (14/05/2018).
Keywords: Aerobic exercise; Anti-cancer mechanisms; Cancer precursors; Cancer risk; Exercise oncology; Resistance exercise.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Dispenzieri A, Katzmann JA, Kyle RA, Larson DR, Melton LJ, Colby CL, et al. Prevalence and risk of progression of light-chain monoclonal gammopathy of undetermined significance: a retrospective population-based cohort study. Lancet. 2010;375(9727):1721–8. doi: 10.1016/S0140-6736(10)60482-5. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
