

Textbook oncologic outcomes are associated with increased overall survival in patients with pancreatic head cancer after undergoing laparoscopic pancreaticoduodenectomy
- PMID: 38317188
- PMCID: PMC10845781
- DOI: 10.1186/s12957-024-03322-8
Textbook oncologic outcomes are associated with increased overall survival in patients with pancreatic head cancer after undergoing laparoscopic pancreaticoduodenectomy
Abstract
Background: Textbook oncologic outcomes (TOO) have been used to evaluate long-term oncologic outcomes for patients after pancreaticoduodenectomy (PD) but not laparoscopic pancreaticoduodenectomy (LPD). The aim of the study was to assess the prognostic value of TOO for patients with pancreatic head cancer undergoing LPD and discuss the risk factors associated with achieving TOO.
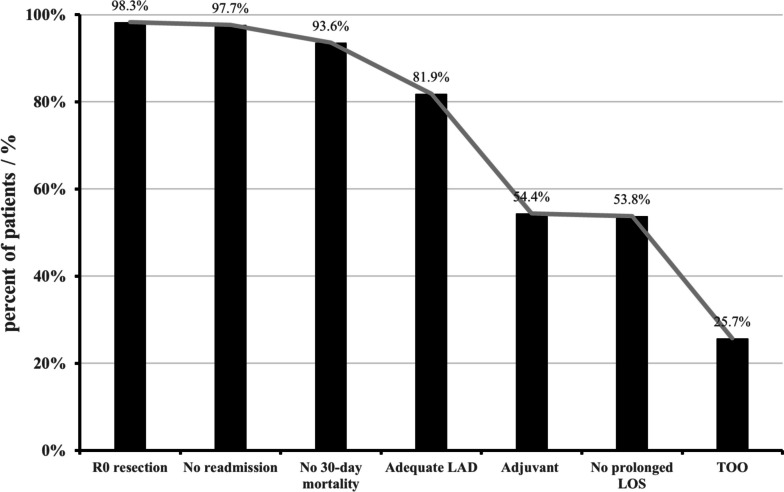
Methods: Patients with pancreatic head cancer who underwent LPD in West China Hospital from January 2015 to May 2022 were consecutively enrolled. TOO was defined as achieving R0 resection, examination of ≥ 12 lymph nodes, no prolonged length of stay, no 30-day readmission/death, and receiving adjuvant chemotherapy. Survival analysis was used to determine the prognostic value of a TOO on overall survival (OS) and recurrence-free survival (RFS). Logistic regression was used to identify the risk factors of a TOO. The rates of a TOO and of each indicator were compared in patients who suffered or not from delayed gastric emptying (DGE).
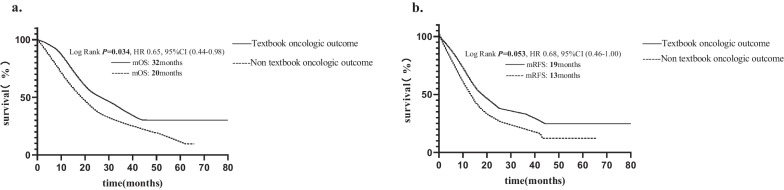
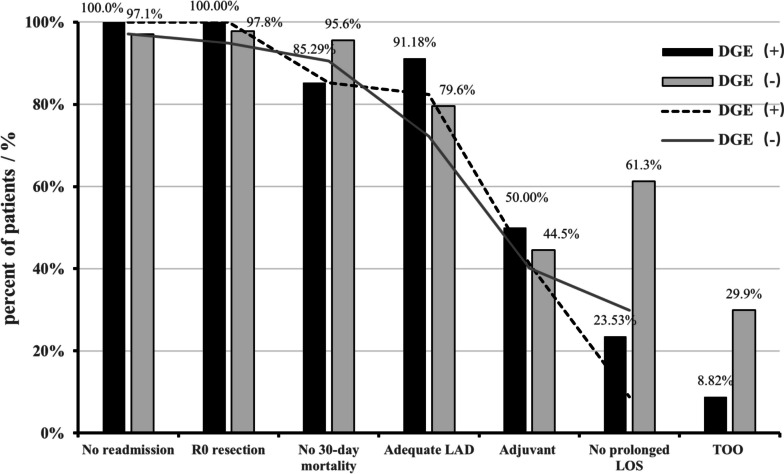
Results: A total of 44 (25.73%) patients achieved TOO which was associated with improved median OS (TOO 32 months vs. non-TOO 20 months, P = 0.034) and a better RFS (TOO 19 months vs. non-TOO 13 months, P = 0.053). Patients suffering from DGE [odds ratio (OR) 4.045, 95% CI 1.151-14.214, P = 0.029] were independent risk factors for TOO. In addition, patients with DGE after surgery had a significantly lower rate of TOO (P = 0.015) than patients without DGE.
Conclusions: As there were significant differences between patients who achieved TOO or not, TOO is a good indicator for long-term oncologic outcomes in patients with pancreatic head cancer after undergoing LPD. DGE is the risk factor for achieving TOO, so it is important to prevent the DGE after LPD to improve the rate of TOO.
Keywords: Laparoscopic pancreaticoduodenectomy; Pancreatic head cancer; Prognosis; Textbook oncologic outcome.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
[Study of perioperative safety of laparoscopic pancreaticoduodenectomy in elderly patients].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2023 Oct;35(10):1063-1069. doi: 10.3760/cma.j.cn121430-20230731-00570. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2023. PMID: 37873711 Chinese.
-
Laparoscopic pancreaticoduodenectomy for tumors of the head of pancreas; 10 cases for a single center experience.Eur Rev Med Pharmacol Sci. 2017 Oct;21(17):3745-3753. Eur Rev Med Pharmacol Sci. 2017. PMID: 28975996
-
[Perioperative efficacy of laparoscopic duodenal-preserving pancreatic head resection].Zhonghua Wai Ke Za Zhi. 2024 Jul 1;62(7):671-676. doi: 10.3760/cma.j.cn112139-20240317-00130. Zhonghua Wai Ke Za Zhi. 2024. PMID: 38808434 Chinese.
-
Is total laparoscopic pancreaticoduodenectomy superior to open procedure? A meta-analysis.World J Gastroenterol. 2019 Oct 7;25(37):5711-5731. doi: 10.3748/wjg.v25.i37.5711. World J Gastroenterol. 2019. PMID: 31602170 Free PMC article.
-
Laparoscopic pancreaticoduodenectomy with portal or superior mesenteric vein resection and reconstruction for pancreatic cancer: A single-center experience.Hepatobiliary Pancreat Dis Int. 2023 Apr;22(2):147-153. doi: 10.1016/j.hbpd.2023.01.004. Epub 2023 Jan 18. Hepatobiliary Pancreat Dis Int. 2023. PMID: 36690522 Review.
Cited by
-
Defining Textbook Outcomes for Minimally Invasive Surgical Resection of Small Gastrointestinal Stromal Tumors (GIST) of the Stomach.Ann Surg Oncol. 2025 Apr;32(4):2951-2957. doi: 10.1245/s10434-024-16714-7. Epub 2025 Jan 3. Ann Surg Oncol. 2025. PMID: 39751981
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
