

Impact of individual level uncertainty of lung cancer polygenic risk score (PRS) on risk stratification
- PMID: 38317189
- PMCID: PMC10840262
- DOI: 10.1186/s13073-024-01298-4
Impact of individual level uncertainty of lung cancer polygenic risk score (PRS) on risk stratification
Abstract
Background: Although polygenic risk score (PRS) has emerged as a promising tool for predicting cancer risk from genome-wide association studies (GWAS), the individual-level accuracy of lung cancer PRS and the extent to which its impact on subsequent clinical applications remains largely unexplored.
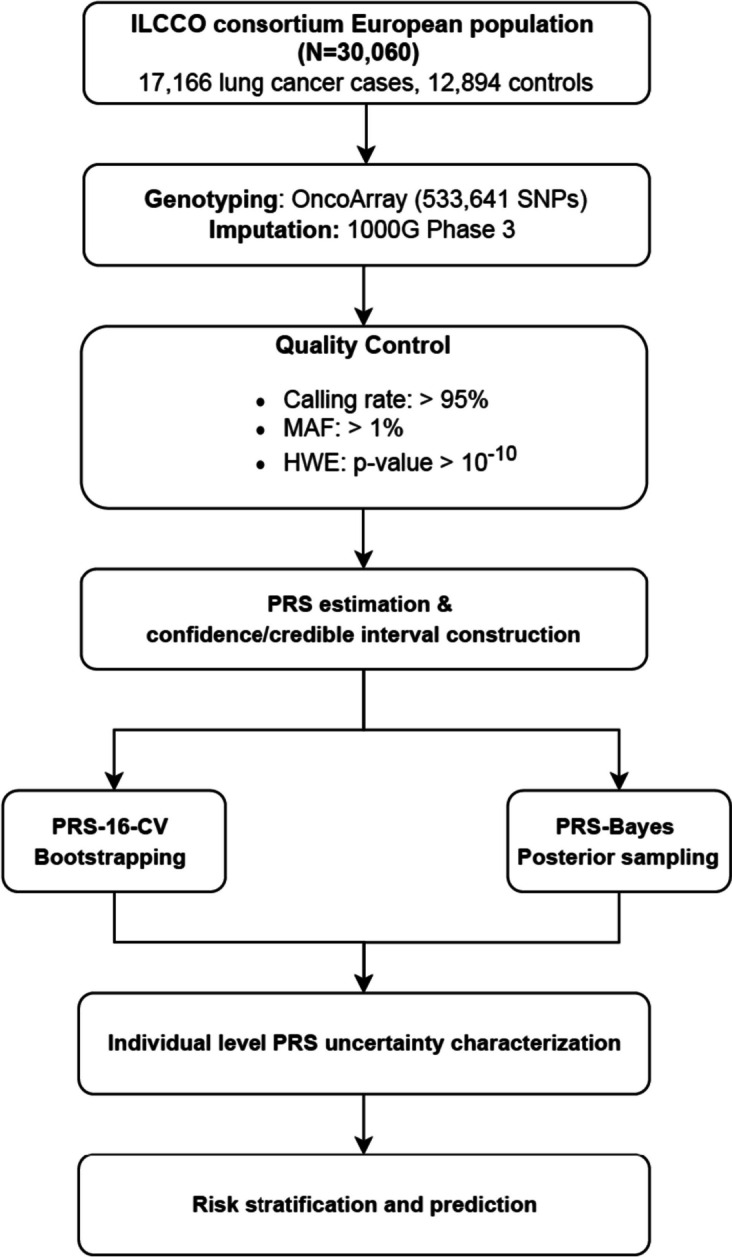
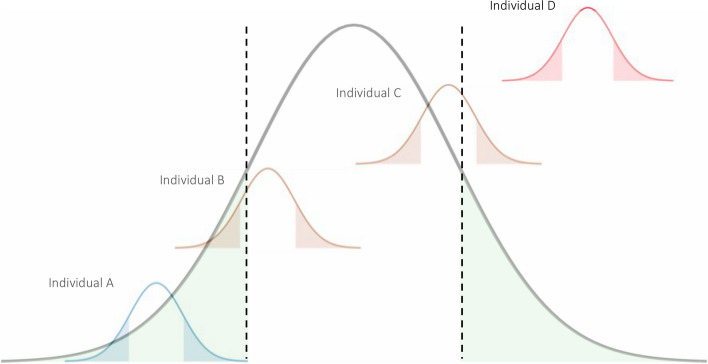
Methods: Lung cancer PRSs and confidence/credible interval (CI) were constructed using two statistical approaches for each individual: (1) the weighted sum of 16 GWAS-derived significant SNP loci and the CI through the bootstrapping method (PRS-16-CV) and (2) LDpred2 and the CI through posteriors sampling (PRS-Bayes), among 17,166 lung cancer cases and 12,894 controls with European ancestry from the International Lung Cancer Consortium. Individuals were classified into different genetic risk subgroups based on the relationship between their own PRS mean/PRS CI and the population level threshold.
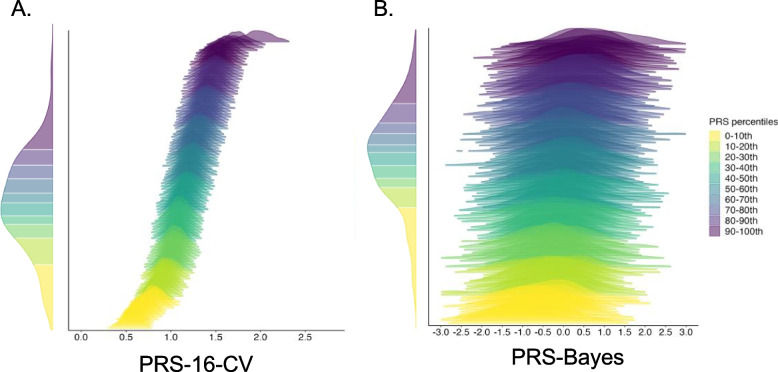
Results: Considerable variances in PRS point estimates at the individual level were observed for both methods, with an average standard deviation (s.d.) of 0.12 for PRS-16-CV and a much larger s.d. of 0.88 for PRS-Bayes. Using PRS-16-CV, only 25.0% of individuals with PRS point estimates in the lowest decile of PRS and 16.8% in the highest decile have their entire 95% CI fully contained in the lowest and highest decile, respectively, while PRS-Bayes was unable to find any eligible individuals. Only 19% of the individuals were concordantly identified as having high genetic risk (> 90th percentile) using the two PRS estimators. An increased relative risk of lung cancer comparing the highest PRS percentile to the lowest was observed when taking the CI into account (OR = 2.73, 95% CI: 2.12-3.50, P-value = 4.13 × 10-15) compared to using PRS-16-CV mean (OR = 2.23, 95% CI: 1.99-2.49, P-value = 5.70 × 10-46). Improved risk prediction performance with higher AUC was consistently observed in individuals identified by PRS-16-CV CI, and the best performance was achieved by incorporating age, gender, and detailed smoking pack-years (AUC: 0.73, 95% CI = 0.72-0.74).
Conclusions: Lung cancer PRS estimates using different methods have modest correlations at the individual level, highlighting the importance of considering individual-level uncertainty when evaluating the practical utility of PRS.
Keywords: Cancer control; Genetic epidemiology; Non-small cell lung cancer (NSCLC); Polygenic risk score (PRSs); Population science.
© 2024. The Author(s).
Conflict of interest statement
M. C. Aldrich reports funding from NIH and GO2 foundation, and she serves an advisor to Guardant Health. While M. Johansson and J. D. McKay are identified as personnel of the International Agency for Research on Cancer/World Health Organization, the authors alone are responsible for the views expressed in this article and they do not necessarily represent the decisions, policy, or views of the International Agency for Research on Cancer/World Health Organization. The remaining authors declare that they have no competing interests.
Figures
Similar articles
-
Large uncertainty in individual polygenic risk score estimation impacts PRS-based risk stratification.Nat Genet. 2022 Jan;54(1):30-39. doi: 10.1038/s41588-021-00961-5. Epub 2021 Dec 20. Nat Genet. 2022. PMID: 34931067 Free PMC article.
-
Identification of risk loci and a polygenic risk score for lung cancer: a large-scale prospective cohort study in Chinese populations.Lancet Respir Med. 2019 Oct;7(10):881-891. doi: 10.1016/S2213-2600(19)30144-4. Epub 2019 Jul 17. Lancet Respir Med. 2019. PMID: 31326317 Free PMC article.
-
Polygenic risk scores for the prediction of common cancers in East Asians: A population-based prospective cohort study.Elife. 2023 Mar 27;12:e82608. doi: 10.7554/eLife.82608. Elife. 2023. PMID: 36971353 Free PMC article.
-
Genome-wide association studies and polygenic risk scores for skin cancer: clinically useful yet?Br J Dermatol. 2019 Dec;181(6):1146-1155. doi: 10.1111/bjd.17917. Epub 2019 Jul 7. Br J Dermatol. 2019. PMID: 30908599 Free PMC article. Review.
-
Polygenic risk scores in atrial fibrillation: Associations and clinical utility in disease prediction.Heart Rhythm. 2024 Jun;21(6):913-918. doi: 10.1016/j.hrthm.2024.02.006. Epub 2024 Feb 7. Heart Rhythm. 2024. PMID: 38336192 Review.
Cited by
-
The causal nexus between diverse smoking statuses, potential therapeutic targets, and NSCLC: insights from Mendelian randomization and mediation analysis.Front Oncol. 2024 Nov 4;14:1438851. doi: 10.3389/fonc.2024.1438851. eCollection 2024. Front Oncol. 2024. PMID: 39558952 Free PMC article.
-
PGSFusion streamlines polygenic score construction and epidemiological applications in biobank-scale cohorts.Genome Med. 2025 Jul 14;17(1):77. doi: 10.1186/s13073-025-01505-w. Genome Med. 2025. PMID: 40653480 Free PMC article.
-
Precision Medicine in Lung Cancer Screening: A Paradigm Shift in Early Detection-Precision Screening for Lung Cancer.Diagnostics (Basel). 2025 Jun 19;15(12):1562. doi: 10.3390/diagnostics15121562. Diagnostics (Basel). 2025. PMID: 40564882 Free PMC article. Review.
-
Attitudes regarding polygenic risk testing for lung cancer: a mixed-methods study.Ann Behav Med. 2025 Jan 4;59(1):kaaf020. doi: 10.1093/abm/kaaf020. Ann Behav Med. 2025. PMID: 40261086
-
PennPRS: a centralized cloud computing platform for efficient polygenic risk score training in precision medicine.medRxiv [Preprint]. 2025 Feb 10:2025.02.07.25321875. doi: 10.1101/2025.02.07.25321875. medRxiv. 2025. PMID: 39990574 Free PMC article. Preprint.
References
-
- Center., A.C.S.C.S . Key statistics for lung cancer. 2022.
-
- Doll R, et al. Mortality in relation to smoking: 50 years' observations on male British doctors. BMJ. 2004;328(7455):1519. doi: 10.1136/bmj.38142.554479.AE. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
