

Long COVID is associated with severe cognitive slowing: a multicentre cross-sectional study
- PMID: 38318123
- PMCID: PMC10839583
- DOI: 10.1016/j.eclinm.2024.102434
Long COVID is associated with severe cognitive slowing: a multicentre cross-sectional study
Abstract
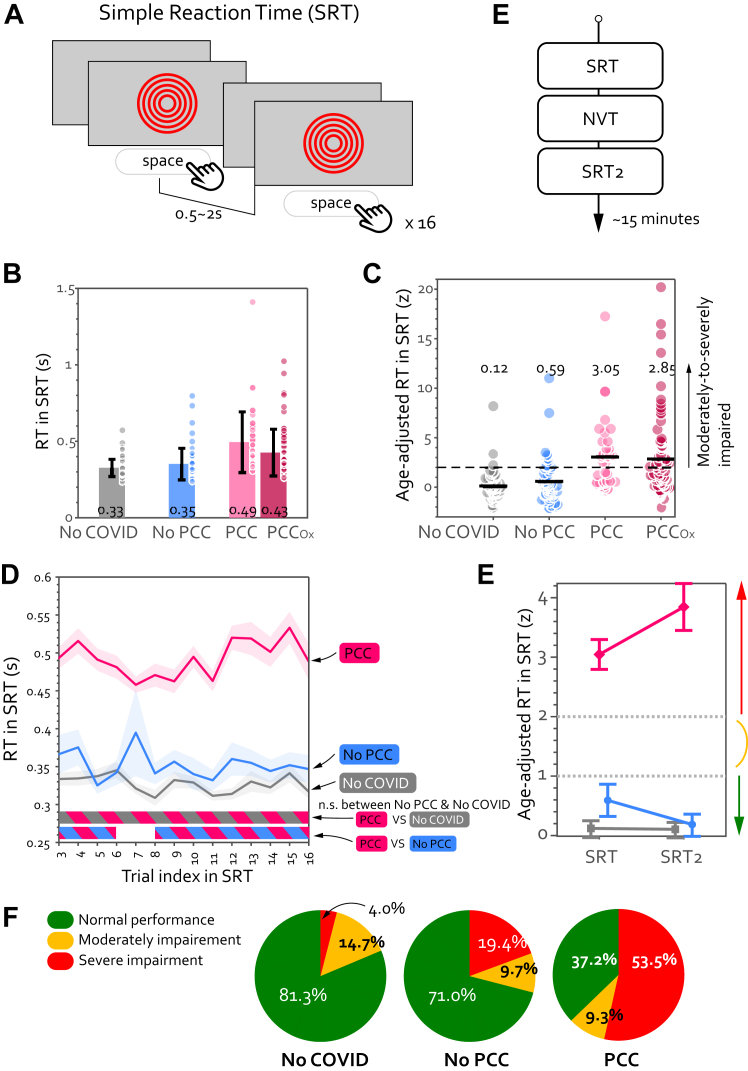
Background: COVID-19 survivors may experience a wide range of chronic cognitive symptoms for months or years as part of post-COVID-19 conditions (PCC). To date, there is no definitive objective cognitive marker for PCC. We hypothesised that a key common deficit in people with PCC might be generalised cognitive slowing.
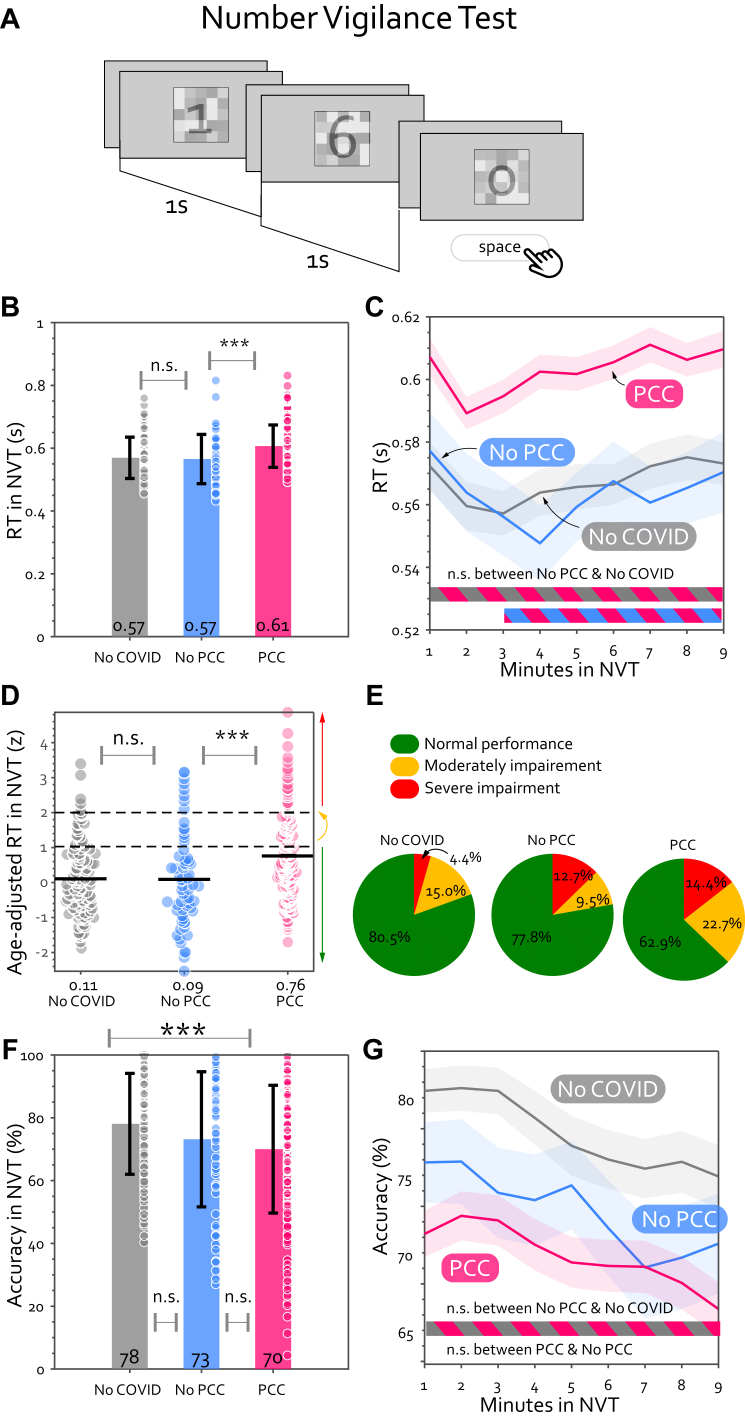
Methods: To examine cognitive slowing, patients with PCC completed two short web-based cognitive tasks, Simple Reaction Time (SRT) and Number Vigilance Test (NVT). 270 patients diagnosed with PCC at two different clinics in UK and Germany were compared to two control groups: individuals who contracted COVID-19 before but did not experience PCC after recovery (No-PCC group) and uninfected individuals (No-COVID group). All patients with PCC completed the study between May 18, 2021 and July 4, 2023 in Jena University Hospital, Jena, Germany and Long COVID clinic, Oxford, UK.
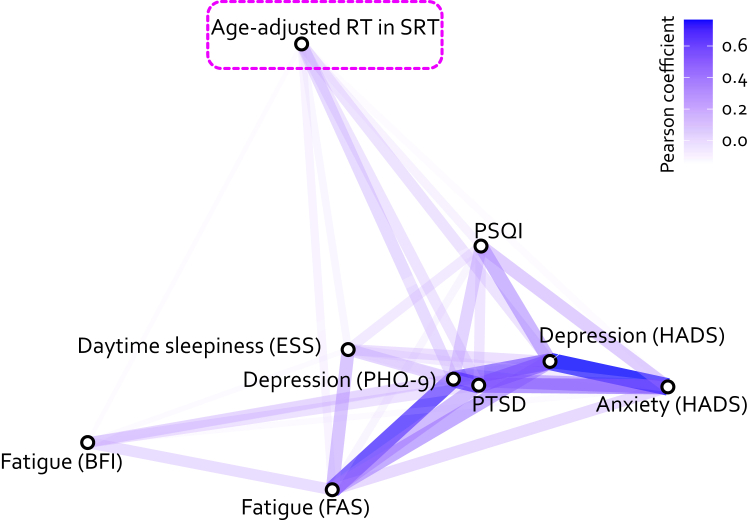
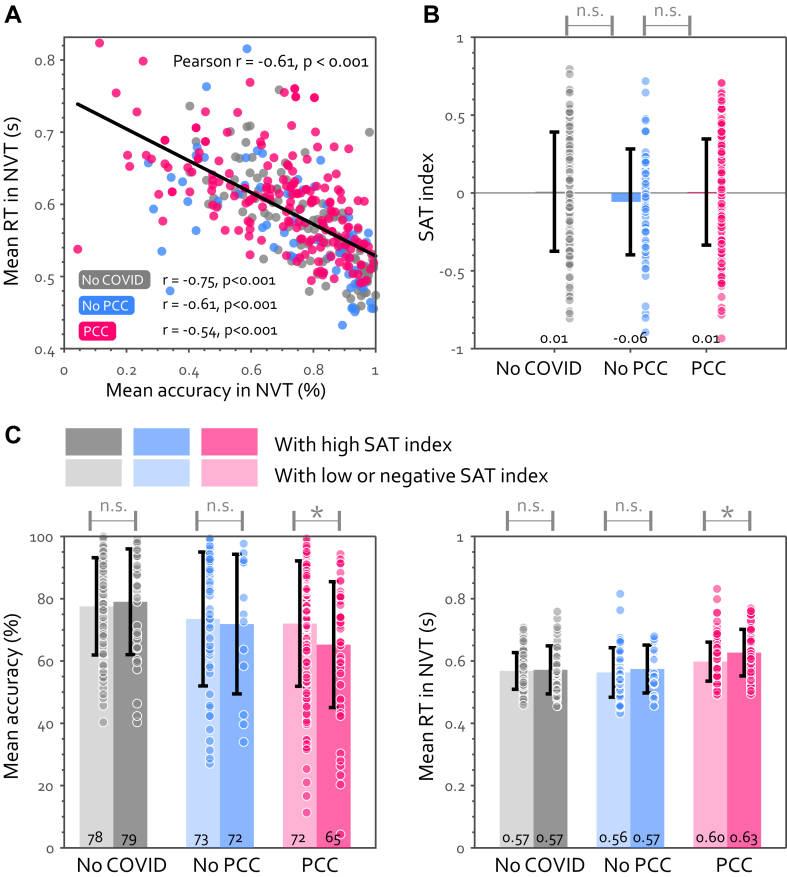
Findings: We identified pronounced cognitive slowing in patients with PCC, which distinguished them from age-matched healthy individuals who previously had symptomatic COVID-19 but did not manifest PCC. Cognitive slowing was evident even on a 30-s task measuring simple reaction time (SRT), with patients with PCC responding to stimuli ∼3 standard deviations slower than healthy controls. 53.5% of patients with PCC's response speed was slower than 2 standard deviations from the control mean, indicating a high prevalence of cognitive slowing in PCC. This finding was replicated across two clinic samples in Germany and the UK. Comorbidities such as fatigue, depression, anxiety, sleep disturbance, and post-traumatic stress disorder did not account for the extent of cognitive slowing in patients with PCC. Furthermore, cognitive slowing on the SRT was highly correlated with the poor performance of patients with PCC on the NVT measure of sustained attention.
Interpretation: Together, these results robustly demonstrate pronounced cognitive slowing in people with PCC, which distinguishes them from age-matched healthy individuals who previously had symptomatic COVID-19 but did not manifest PCC. This might be an important factor contributing to some of the cognitive impairments reported in patients with PCC.
Funding: Wellcome Trust (206330/Z/17/Z), NIHR Oxford Health Biomedical Research Centre, the Thüringer Aufbaubank (2021 FGI 0060), German Forschungsgemeinschaft (DFG, FI 1424/2-1) and the Horizon 2020 Framework Programme of the European Union (ITN SmartAge, H2020-MSCA-ITN-2019-859890).
Keywords: COVID-19; Cognition; Post-COVID conditions; Post-acute COVID syndrome; Processing speed; Response time.
© 2024 The Author(s).
Conflict of interest statement
All authors declare no financial or non-financial competing interests.
Figures

References
-
- World Health Organization . World Health Organization; 2021. A clinical case definition of post COVID-19 condition by a Delphi consensus, 6 October 2021.https://apps.who.int/iris/handle/10665/345824 Accessed May 12, 2023.
Grants and funding
LinkOut - more resources
Full Text Sources
