

Early Immune Remodeling Steers Clinical Response to First-Line Chemoimmunotherapy in Advanced Gastric Cancer
- PMID: 38319303
- PMCID: PMC11061611
- DOI: 10.1158/2159-8290.CD-23-0857
Early Immune Remodeling Steers Clinical Response to First-Line Chemoimmunotherapy in Advanced Gastric Cancer
Abstract
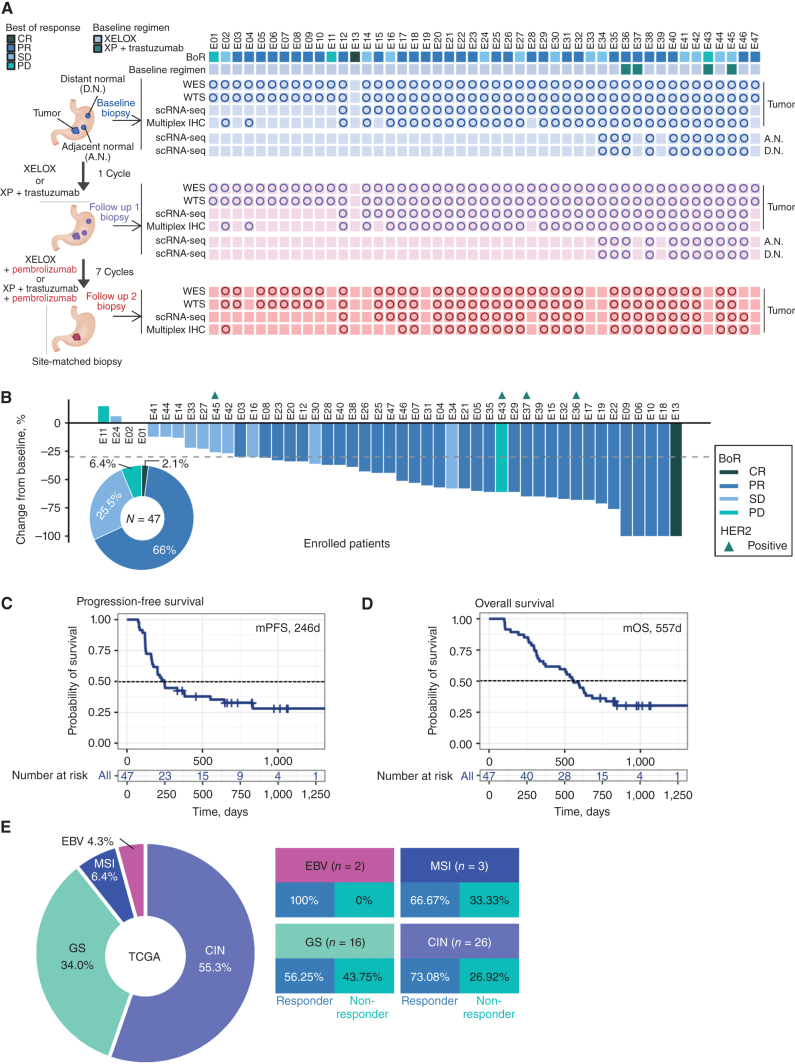
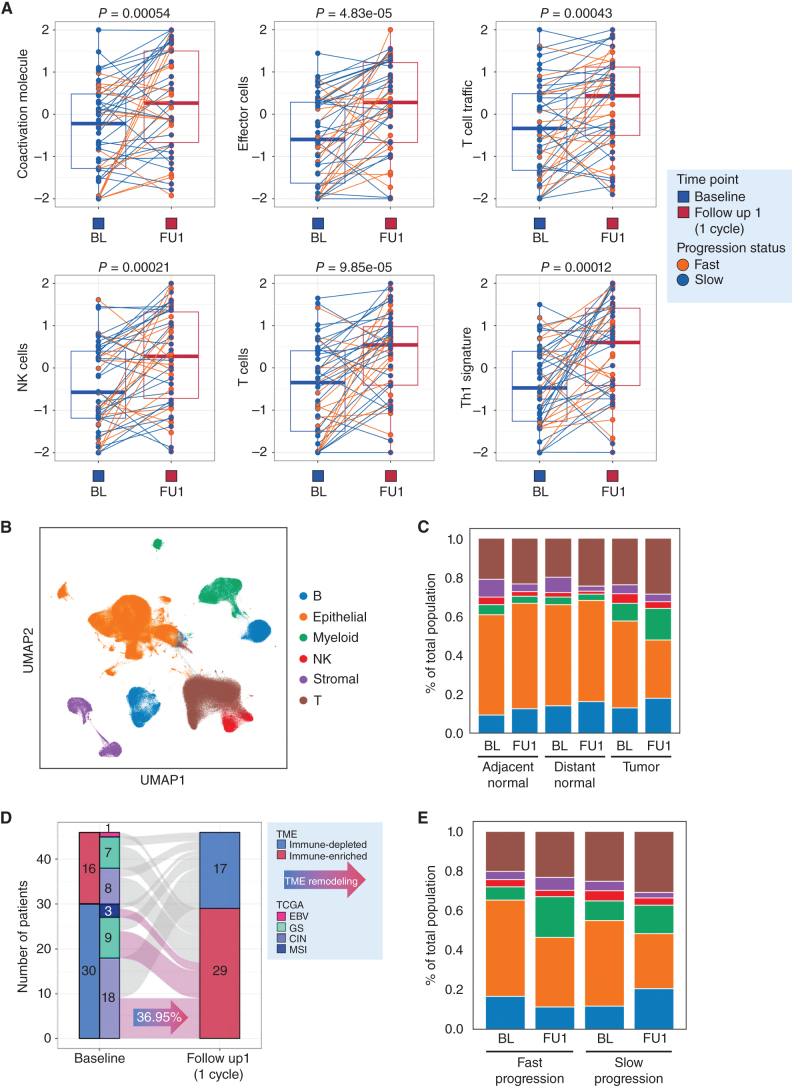
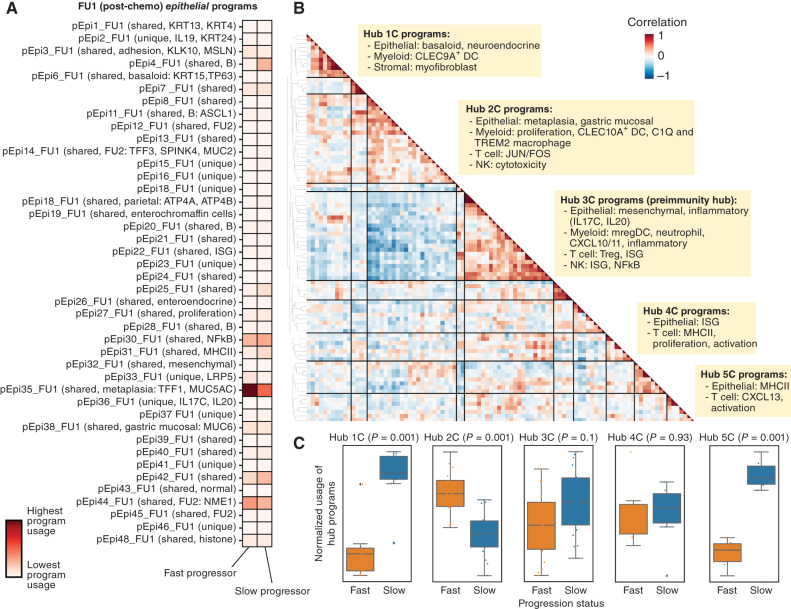
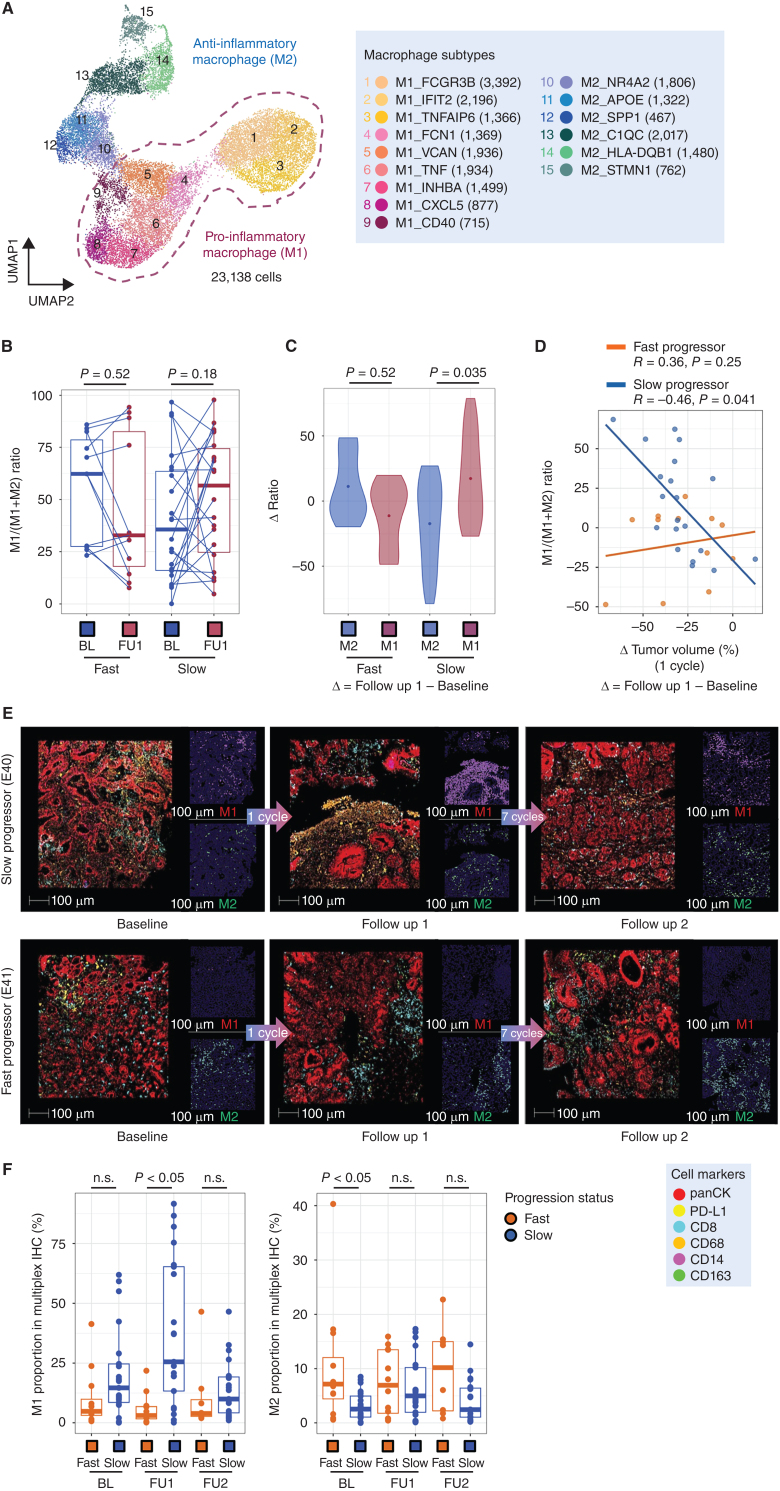
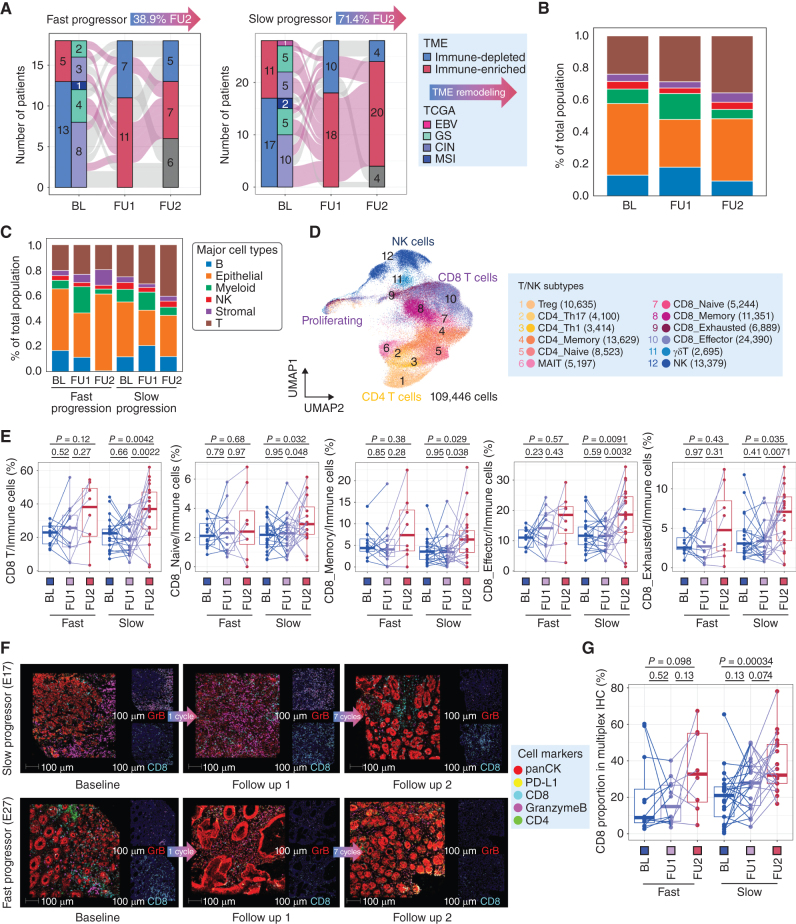
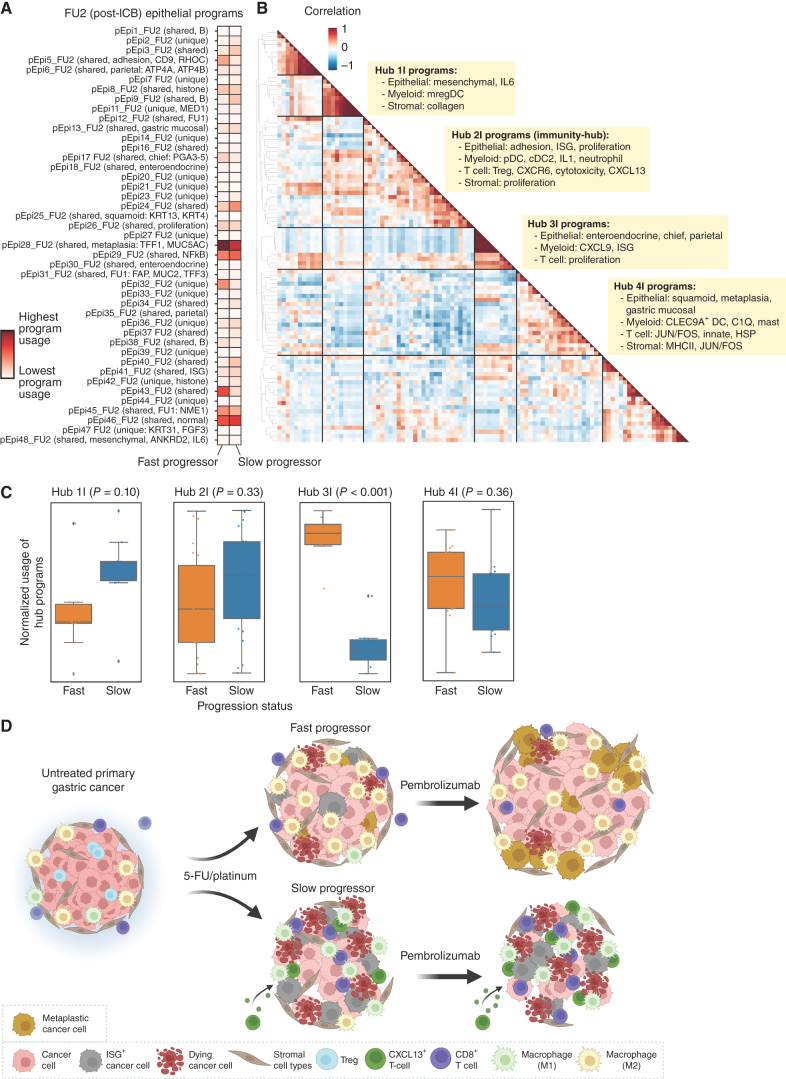
Adding anti-programmed cell death protein 1 (anti-PD-1) to 5-fluorouracil (5-FU)/platinum improves survival in some advanced gastroesophageal adenocarcinomas (GEA). To understand the effects of chemotherapy and immunotherapy, we conducted a phase II first-line trial (n = 47) sequentially adding pembrolizumab to 5-FU/platinum in advanced GEA. Using serial biopsy of the primary tumor at baseline, after one cycle of 5-FU/platinum, and after the addition of pembrolizumab, we transcriptionally profiled 358,067 single cells to identify evolving multicellular tumor microenvironment (TME) networks. Chemotherapy induced early on-treatment multicellular hubs with tumor-reactive T-cell and M1-like macrophage interactions in slow progressors. Faster progression featured increased MUC5A and MSLN containing treatment resistance programs in tumor cells and M2-like macrophages with immunosuppressive stromal interactions. After pembrolizumab, we observed increased CD8 T-cell infiltration and development of an immunity hub involving tumor-reactive CXCL13 T-cell program and epithelial interferon-stimulated gene programs. Strategies to drive increases in antitumor immune hub formation could expand the portion of patients benefiting from anti-PD-1 approaches.
Significance: The benefit of 5-FU/platinum with anti-PD-1 in first-line advanced gastric cancer is limited to patient subgroups. Using a trial with sequential anti-PD-1, we show coordinated induction of multicellular TME hubs informs the ability of anti-PD-1 to potentiate T cell-driven responses. Differential TME hub development highlights features that underlie clinical outcomes. This article is featured in Selected Articles from This Issue, p. 695.
©2024 The Authors; Published by the American Association for Cancer Research.
Figures
References
-
- Yoon HH, Jin Z, Kour O, Kankeu Fonkoua LA, Shitara K, Gibson MK, et al. . Association of PD-L1 expression and other variables with benefit from immune checkpoint inhibition in advanced gastroesophageal cancer: systematic review and meta-analysis of 17 phase 3 randomized clinical trials. JAMA Oncol 2022;8:1456–65. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
