

Smoking Status and Survival in Patients With Early-Stage Primary Cutaneous Melanoma
- PMID: 38319662
- PMCID: PMC10848058
- DOI: 10.1001/jamanetworkopen.2023.54751
Smoking Status and Survival in Patients With Early-Stage Primary Cutaneous Melanoma
Abstract
Importance: While smoking is associated with a decreased incidence of cutaneous melanoma, the association of smoking with melanoma progression and death is not well defined.
Objective: To determine the association of smoking with survival in patients with early-stage primary cutaneous melanoma.
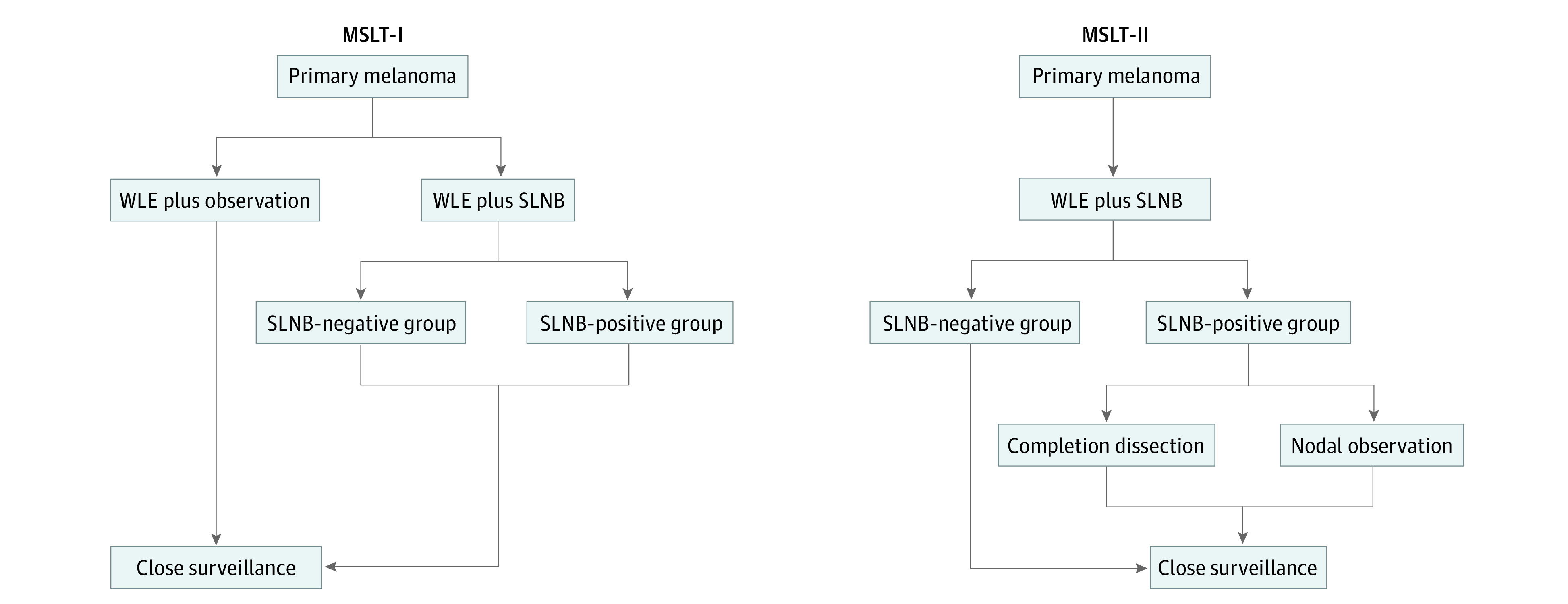
Design, setting, and participants: This cohort study performed a post hoc analysis of data derived from the randomized, multinational first and second Multicenter Selective Lymphadenectomy Trials (MSLT-I and MSLT-II). Participants were accrued for MSLT-I from January 20, 1994, to March 29, 2002; MSLT-II, from December 21, 2004, to March 31, 2014. Median follow-up was 110.0 (IQR, 53.4-120.0) months for MSLT-I and 67.6 (IQR, 25.8-110.2) months for MSLT-II. Patients aged 18 to 75 years with clinical stages I or II melanoma with a Breslow thickness of 1.00 mm or greater or Clark level IV to V and available standard prognostic and smoking data were included. Analyses were performed from October 4, 2022, to March 31, 2023.
Exposure: Current, former, and never smoking.
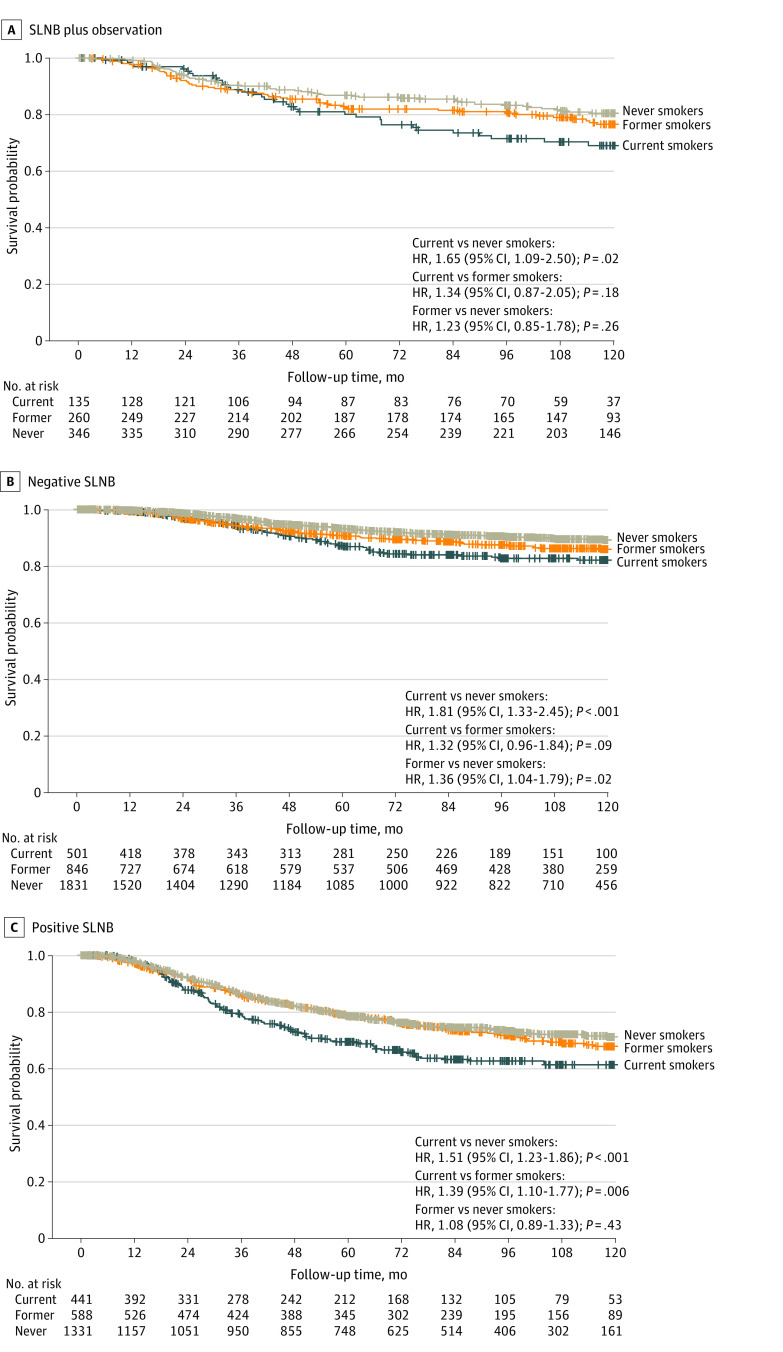
Main outcomes and measures: Melanoma-specific survival of patients with current, former, and never smoking status was assessed for the entire cohort and for nodal observation and among subgroups with sentinel lymph node biopsy (SLNB)-negative and SLNB-positive findings.
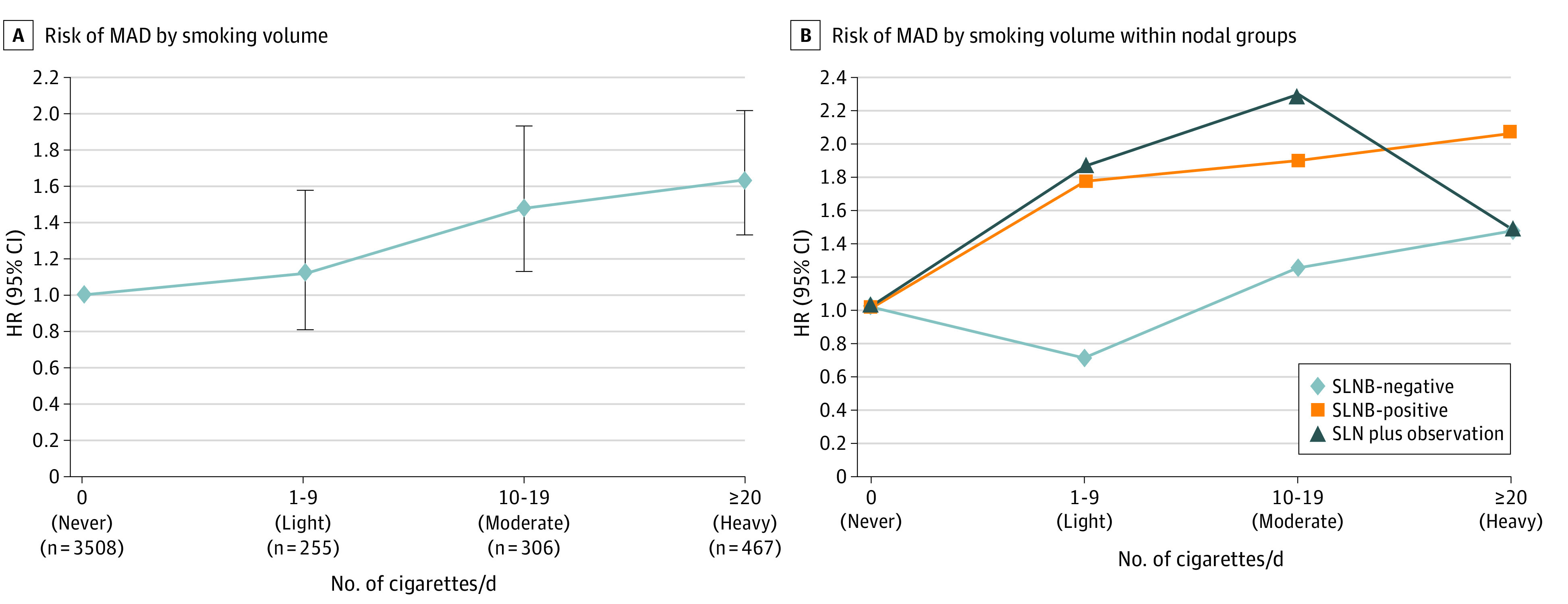
Results: Of 6279 included patients, 3635 (57.9%) were men, and mean (SD) age was 52.7 (13.4) years. The most common tumor location was an extremity (2743 [43.7%]), and mean (SD) Breslow thickness was 2.44 (2.06) mm. Smoking status included 1077 (17.2%) current, 1694 (27.0%) former, and 3508 (55.9%) never. Median follow-up was 78.4 (IQR, 30.5-119.6) months. Current smoking was associated with male sex, younger age, trunk site, thicker tumors, tumor ulceration, and SLNB positivity. Current smoking was associated with a greater risk of melanoma-associated death by multivariable analysis for the entire study (hazard ratio [HR], 1.48 [95% CI, 1.26-1.75]; P < .001). Former smoking was not. The increased risk of melanoma-specific mortality associated with current smoking was greatest for patients with SLNB-negative melanoma (HR, 1.85 [95% CI, 1.35-2.52]; P < .001), but also present for patients with SLNB-positive melanoma (HR, 1.29 [95% CI, 1.04-1.59]; P = .02) and nodal observation (HR, 1.68 [95% CI, 1.09-2.61]; P = .02). Smoking at least 20 cigarettes/d doubled the risk of death due to melanoma for patients with SLNB-negative disease (HR, 2.06 [95% CI, 1.36-3.13]; P < .001).
Conclusions and relevance: The findings of this cohort study suggest that patients with clinical stage I and II melanoma who smoked had a significantly increased risk of death due to melanoma. Smoking status should be assessed at time of melanoma diagnosis and may be considered a risk factor for disease progression.
Conflict of interest statement
Figures
Comment in
-
Smoking and Melanoma Outcomes-Another Reason to Quit.JAMA Netw Open. 2024 Feb 5;7(2):e2354762. doi: 10.1001/jamanetworkopen.2023.54762. JAMA Netw Open. 2024. PMID: 38319664 No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
