

Comparison of ESIN and other minimally invasive techniques for anterior pelvic ring injury: a finite element analysis and case-control study
- PMID: 38320104
- PMCID: PMC11093452
- DOI: 10.1097/JS9.0000000000001137
Comparison of ESIN and other minimally invasive techniques for anterior pelvic ring injury: a finite element analysis and case-control study
Abstract
Object: A novel technique, percutaneous elastic stable intramedullary nail fixation (ESIN), proposed by our team for the treatment of anterior pelvic ring injury. Finite element analysis and retrospective case-control study were used to compare biomechanical properties and clinical outcomes between ESIN and other techniques.
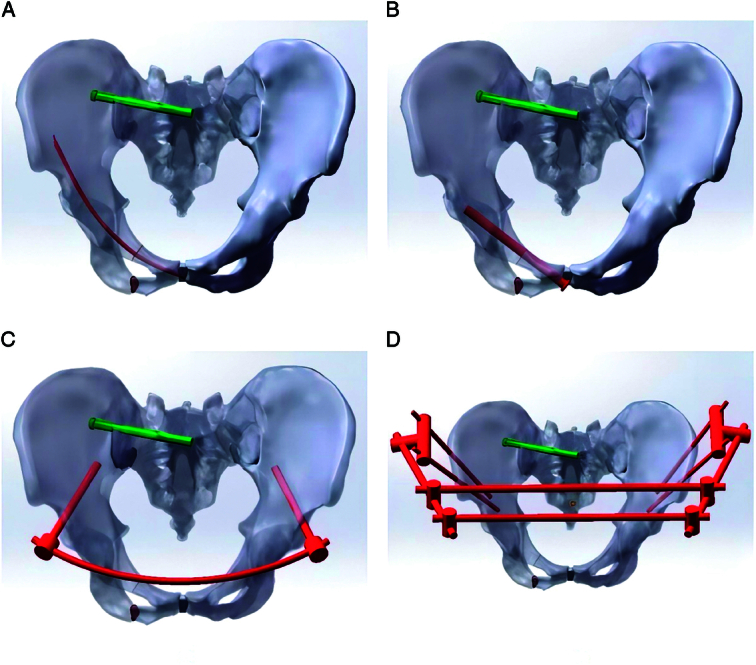
Methods: Four groups of finite element models of pelvic anterior ring injury were simulated, including ESIN (model A), retrograde transpubic screw fixation (RTSF, model B), subcutaneous internal fixator (model C), and external fixator (model D), and a vertical downward load of 500 N was applied to the S1 vertebral endplate. Stress and displacement distributions of intact pelvis, displacement distributions of pubic fracture fragments, and stress distributions of fixation devices were analysed. Then 31 patients with anterior pelvic ring injury (15 in the ESIN group and 16 in the RTSF group) were reviewed. Clinical outcomes were evaluated at the final follow-up. Postoperative complications were also recorded.
Results: Under 500N loading, the intact stability of the pelvis was compared as follows: model B (20.58 mm, 121.82 MPa), model A (20.80 mm, 129.97 MPa), model C (22.02 mm, 141.70 MPa), and model D (22.57 mm, 147.06 MPa). The regional stability of superior pubic ramus was compared as follows: model B (9.48 mm), model A (10.16 mm), model C (10.52 mm), and model D (10.76 mm). All 31 patients received follow-up at least 12 months postsurgery (range 12-20 months). Age, sex, injury mechanism, fracture type, time between the injury and operation, American Society of Anesthesiologists score, intraoperative blood loss, hospital stay, follow-up period, time to union, and Majeed scores did not differ significantly between the two groups ( P >0.05). However, the differences in the duration of unilateral surgery, unilateral intraoperative fluoroscopy and one-time success rate were significant ( P <0.05).
Conclusions: With sufficient biomechanical stability and minimally invasive advantage, the percutaneous technique using ESIN can be used to successfully treat anterior pelvic ring injuries. In addition, advantages over RTSF include a shorter duration of surgery, reduced requirement for intraoperative fluoroscopy, and a higher one-time success rate. ESIN therefore constitutes a good alternative to RTSF.
Copyright © 2024 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors have no relevant financial or nonfinancial interests to disclose.
Figures








Similar articles
-
Finite element analysis of the modified intramedullary nail-II for managing reverse obliquity trochanteric fractures.Sci Rep. 2025 Jul 1;15(1):21303. doi: 10.1038/s41598-025-05748-w. Sci Rep. 2025. PMID: 40595997 Free PMC article.
-
Clinical efficacy and biomechanical analysis of robotic internal fixation with percutaneous screws in the treatment of both-column acetabular fractures.Sci Rep. 2025 Jul 2;15(1):22908. doi: 10.1038/s41598-025-06168-6. Sci Rep. 2025. PMID: 40596294 Free PMC article.
-
Does spinopelvic alignment affect fixation stability in pelvic ring fractures?: A finite element study.Clin Biomech (Bristol). 2025 Aug;128:106622. doi: 10.1016/j.clinbiomech.2025.106622. Epub 2025 Jul 16. Clin Biomech (Bristol). 2025. PMID: 40684733
-
Outcomes and complications of the INFIX technique for unstable pelvic ring injuries with high-velocity trauma: a systematic review and meta-analysis.Arch Orthop Trauma Surg. 2022 May;142(5):787-803. doi: 10.1007/s00402-020-03742-7. Epub 2021 Jan 11. Arch Orthop Trauma Surg. 2022. PMID: 33426606
-
Cephalomedullary nails versus extramedullary implants for extracapsular hip fractures in older adults.Cochrane Database Syst Rev. 2022 Jan 26;1(1):CD000093. doi: 10.1002/14651858.CD000093.pub6. Cochrane Database Syst Rev. 2022. PMID: 35080771 Free PMC article.
Cited by
-
The role of GZMA as a target of cysteine and biomarker in Alzheimer's disease, pelvic organ prolapse, and tumor progression.Front Pharmacol. 2024 Aug 20;15:1447605. doi: 10.3389/fphar.2024.1447605. eCollection 2024. Front Pharmacol. 2024. PMID: 39228516 Free PMC article.
-
Comparison of elastic stable intramedullary nailing versus retrograde screw fixation for pubic ramus fractures-a biomechanical study.Eur J Trauma Emerg Surg. 2025 Mar 8;51(1):129. doi: 10.1007/s00068-025-02791-0. Eur J Trauma Emerg Surg. 2025. PMID: 40057598 Free PMC article.
-
Targeting exercise-related genes and placental growth factor for therapeutic development in head and neck squamous cell carcinoma.Front Pharmacol. 2024 Oct 4;15:1476076. doi: 10.3389/fphar.2024.1476076. eCollection 2024. Front Pharmacol. 2024. PMID: 39431157 Free PMC article.
References
-
- Cole PA, Gauger EM, Anavian J, et al. . Anterior pelvic external fixator versus subcutaneous internal fixator in the treatment of anterior ring pelvic fractures. J Orthop Trauma 2012;26:269–277. - PubMed
-
- Studer P, Suhm N, Zappe B, et al. . Pubic rami fractures in the elderly–a neglected injury? Swiss Med Wkly 2013;143:w13859. - PubMed
-
- Krappinger D, Struve P, Schmid R, et al. . Fractures of the pubic rami: a retrospective review of 534 cases. Arch Orthop Trauma Surg 2009;129:1685–1690. - PubMed
-
- Lee C, Sciadini M. The use of external fixation for the management of the unstable anterior pelvic ring. J Orthop Trauma 2018;32(Suppl 6):S14–s7. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
