

Artificial Intelligence Predictive Model for Hormone Therapy Use in Prostate Cancer
- PMID: 38320143
- PMCID: PMC11195914
- DOI: 10.1056/EVIDoa2300023
Artificial Intelligence Predictive Model for Hormone Therapy Use in Prostate Cancer
Abstract
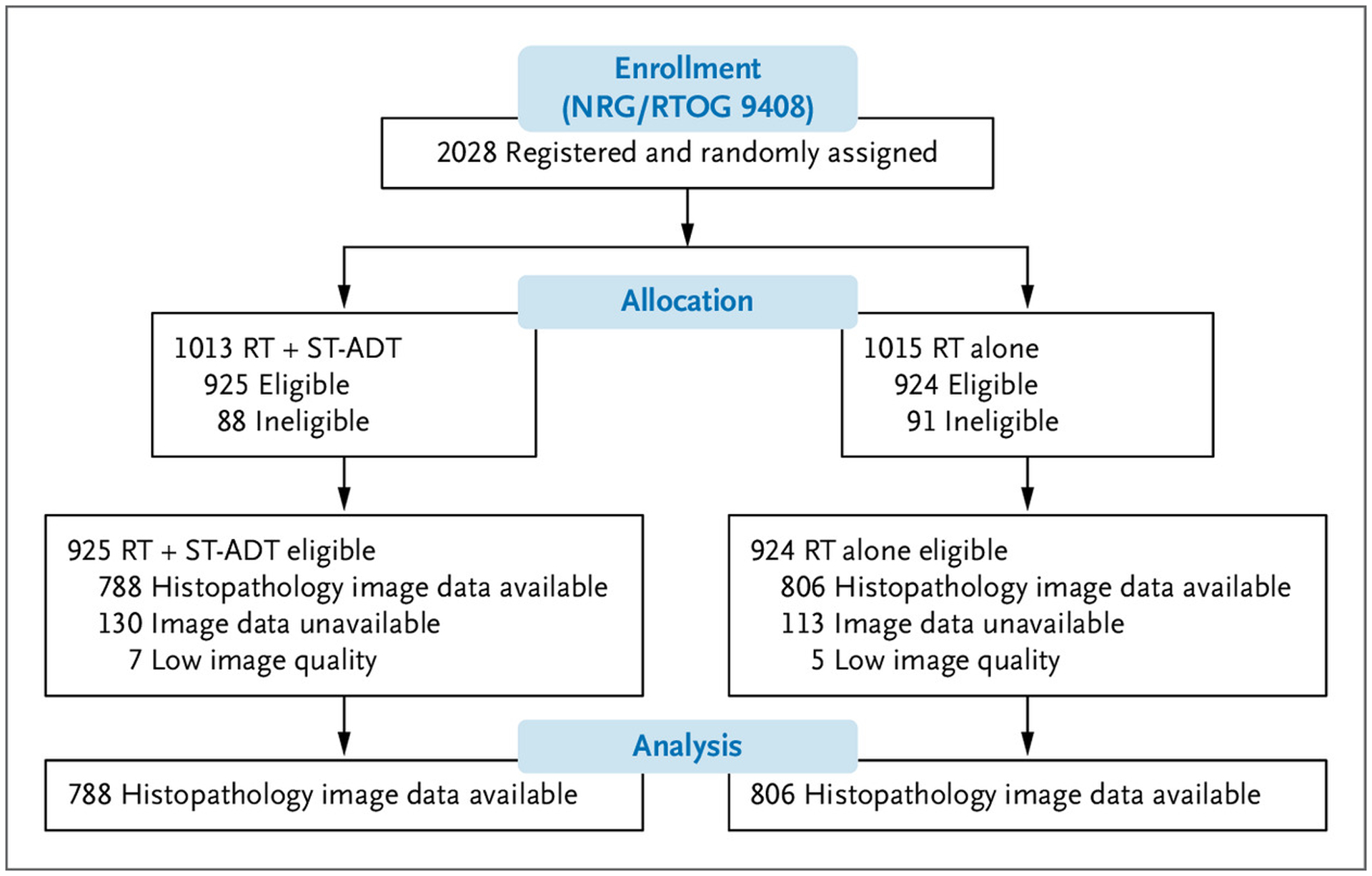
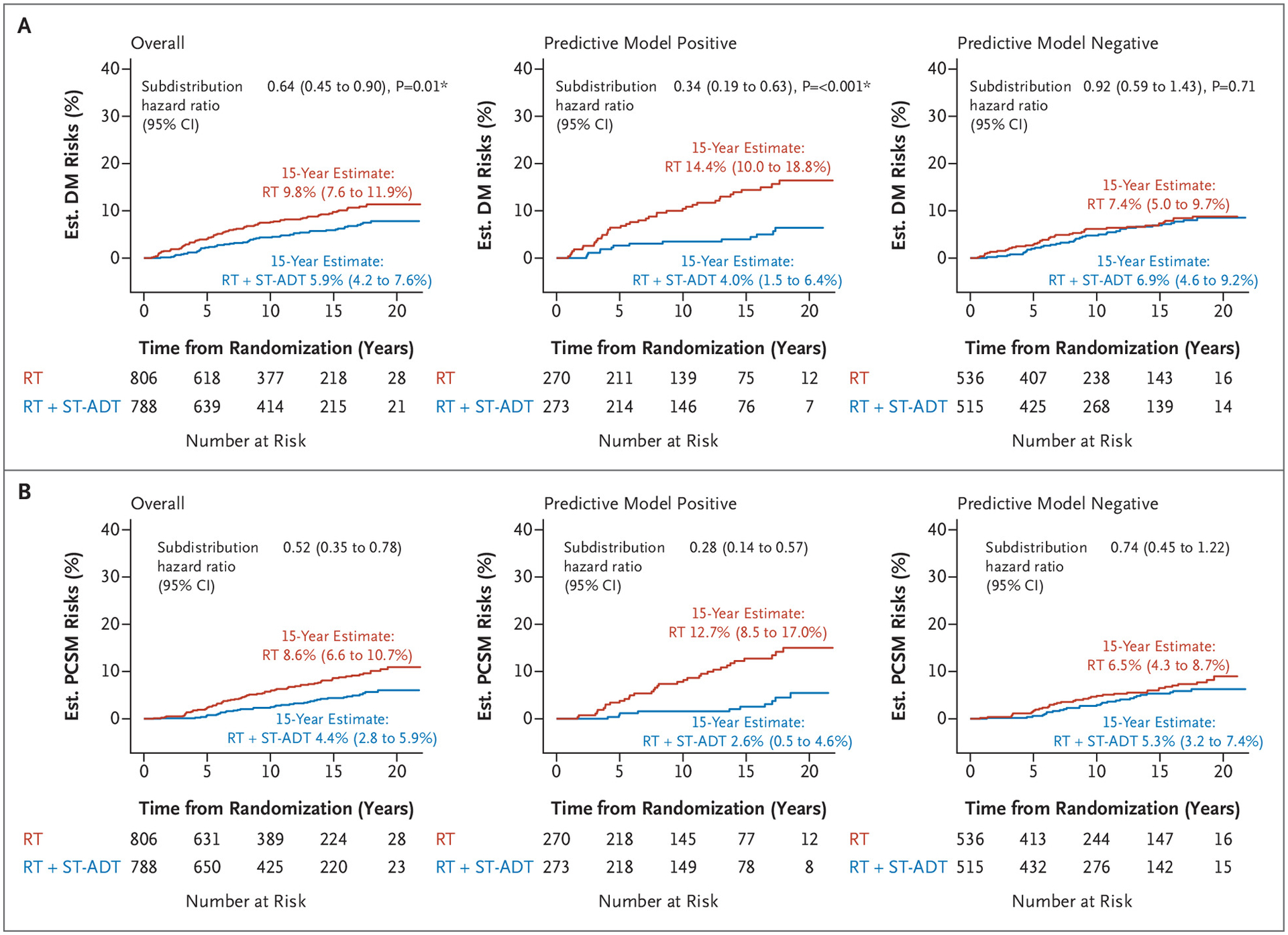
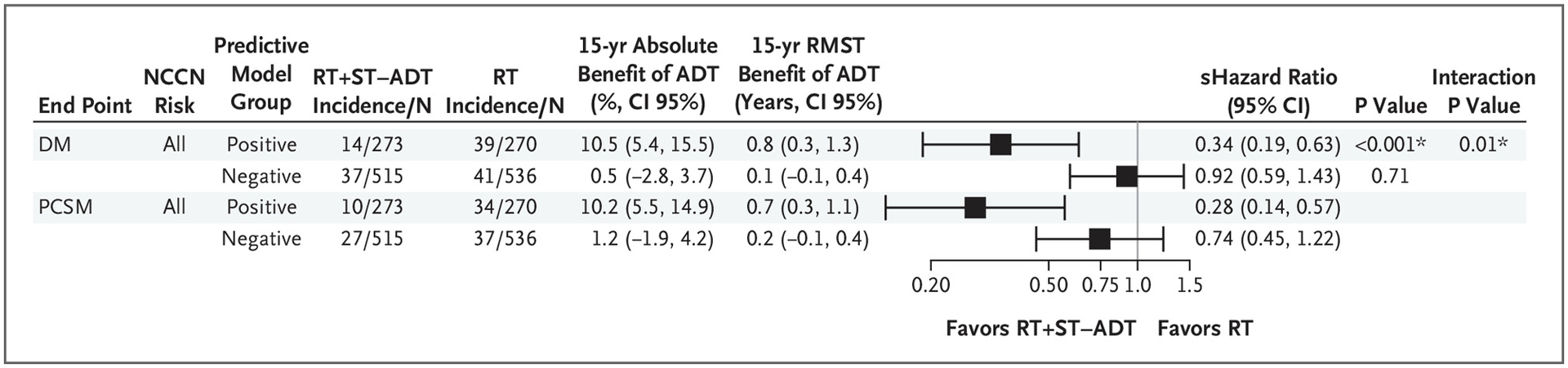
BACKGROUND: Androgen deprivation therapy (ADT) with radiotherapy can benefit patients with localized prostate cancer. However, ADT can negatively impact quality of life, and there remain no validated predictive models to guide its use. METHODS: We used digital pathology images from pretreatment prostate tissue and clinical data from 5727 patients enrolled in five phase 3 randomized trials, in which treatment was radiotherapy with or without ADT, as our data source to develop and validate an artificial intelligence (AI)–derived predictive patient-specific model that would determine which patients would develop the primary end point of distant metastasis. The model used baseline data to provide a binary output that a given patient will likely benefit from ADT or not. After the model was locked, validation was performed using data from NRG Oncology/Radiation Therapy Oncology Group (RTOG) 9408 (n=1594), a trial that randomly assigned men to radiotherapy plus or minus 4 months of ADT. Fine–Gray regression and restricted mean survival times were used to assess the interaction between treatment and the predictive model and within predictive model–positive, i.e., benefited from ADT, and –negative subgroup treatment effects. RESULTS: Overall, in the NRG/RTOG 9408 validation cohort (14.9 years of median follow-up), ADT significantly improved time to distant metastasis. Of these enrolled patients, 543 (34%) were model positive, and ADT significantly reduced the risk of distant metastasis compared with radiotherapy alone. Of 1051 patients who were model negative, ADT did not provide benefit. CONCLUSIONS: Our AI-based predictive model was able to identify patients with a predominantly intermediate risk for prostate cancer likely to benefit from short-term ADT. (Supported by a grant [U10CA180822] from NRG Oncology Statistical and Data Management Center, a grant [UG1CA189867] from NCI Community Oncology Research Program, a grant [U10CA180868] from NRG Oncology Operations, and a grant [U24CA196067] from NRG Specimen Bank from the National Cancer Institute and by Artera, Inc. ClinicalTrials.gov numbers NCT00767286, NCT00002597, NCT00769548, NCT00005044, and NCT00033631.)
Figures
Update of
-
Artificial Intelligence Predictive Model for Hormone Therapy Use in Prostate Cancer.Res Sq [Preprint]. 2023 Apr 21:rs.3.rs-2790858. doi: 10.21203/rs.3.rs-2790858/v1. Res Sq. 2023. Update in: NEJM Evid. 2023 Aug;2(8):EVIDoa2300023. doi: 10.1056/EVIDoa2300023. PMID: 37131691 Free PMC article. Updated. Preprint.
References
-
- Jones CU, Pugh SL, Sandler HM, et al. Adding short-term androgen deprivation therapy to radiation therapy in men with localized prostate cancer: long-term update of the NRG/RTOG 9408 randomized clinical trial [published correction appears in Int J Radiat Oncol Biol Phys 2023;115:265]. Int J Radiat Oncol Biol Phys 2022;112:294–303. DOI: 10.1016/j.ijrobp.2021.08.031. - DOI - PMC - PubMed
-
- Kishan AU, Sun Y, Hartman H, et al. Androgen deprivation therapy use and duration with definitive radiotherapy for localised prostate cancer: an individual patient data meta-analysis [published correction appears in Lancet Oncol 2022;23:e319]. Lancet Oncol 2022;23: 304–316. DOI: 10.1016/S1470-2045(21)00705-1. - DOI - PubMed
