

A Day 14 Endpoint for Acute GVHD Clinical Trials
- PMID: 38320730
- PMCID: PMC11009039
- DOI: 10.1016/j.jtct.2024.01.079
A Day 14 Endpoint for Acute GVHD Clinical Trials
Abstract
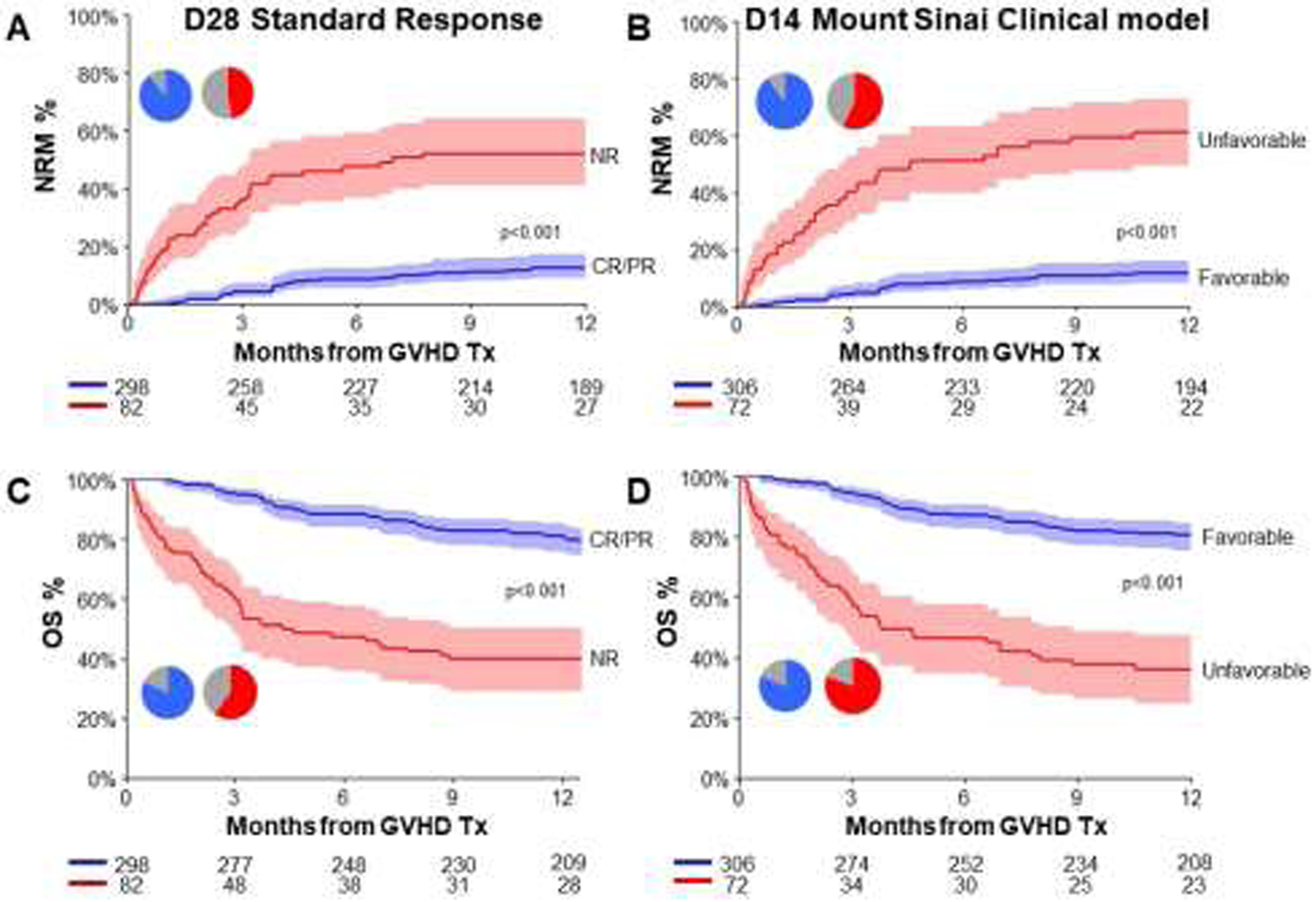
The overall response rate (ORR) 28 days after treatment has been adopted as the primary endpoint for clinical trials of acute graft versus host disease (GVHD). However, physicians often need to modify immunosuppression earlier than day (D) 28, and non-relapse mortality (NRM) does not always correlate with ORR at D28. We studied 1144 patients that received systemic treatment for GVHD in the Mount Sinai Acute GVHD International Consortium (MAGIC) and divided them into a training set (n=764) and a validation set (n=380). We used a recursive partitioning algorithm to create a Mount Sinai model that classifies patients into favorable or unfavorable groups that predicted 12 month NRM according to overall GVHD grade at both onset and D14. In the Mount Sinai model grade II GVHD at D14 was unfavorable for grade III/IV GVHD at onset and predicted NRM as well as the D28 standard response model. The MAGIC algorithm probability (MAP) is a validated score that combines the serum concentrations of suppression of tumorigenicity 2 (ST2) and regenerating islet-derived 3-alpha (REG3α) to predict NRM. Inclusion of the D14 MAP biomarker score with the D14 Mount Sinai model created three distinct groups (good, intermediate, poor) with strikingly different NRM (8%, 35%, 76% respectively). This D14 MAGIC model displayed better AUC, sensitivity, positive and negative predictive value, and net benefit in decision curve analysis compared to the D28 standard response model. We conclude that this D14 MAGIC model could be useful in therapeutic decisions and may offer an improved endpoint for clinical trials of acute GVHD treatment.
Keywords: Acute GVHD; Biomarkers; Classification and regression tree; Competing risk; Competing risks; Composite; Decision curve analysis; Endpoints; Immunosuppression; Machine learning; Nonrelapse mortality; Surrogate; Time-dependent AUC; Treatment response.
Copyright © 2024 The American Society for Transplantation and Cellular Therapy. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures




References
-
- Hahn T, Sucheston-Campbell LE, Preus L, Zhu X, Hansen JA, Martin PJ, et al. Establishment of Definitions and Review Process for Consistent Adjudication of Cause-specific Mortality after Allogeneic Unrelated-donor Hematopoietic Cell Transplantation. Biol Blood Marrow Transplant. 2015;21(9):1679–86. - PMC - PubMed
-
- MacMillan ML, DeFor TE, Weisdorf DJ. The best endpoint for acute GVHD treatment trials. Blood. 2010;115(26):5412–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
