

Investigating the relationship between FRailty And Quality of LIfe in patients with heart faiLure and CKD (FRAIL study)
- PMID: 38320815
- PMCID: PMC11098643
- DOI: 10.1002/ehf2.14693
Investigating the relationship between FRailty And Quality of LIfe in patients with heart faiLure and CKD (FRAIL study)
Abstract
Aims: Patients with chronic kidney disease (CKD) or heart failure (HF) are disproportionally affected by frailty, an independent predictor of morbidity. The prevalence of frailty and its impact on quality of life (QoL) in a unique population of patients with both CKD and HF (CKD-HF) is unclear. The aim of this study was to investigate the association between frailty and QoL in patients with CKD-HF.
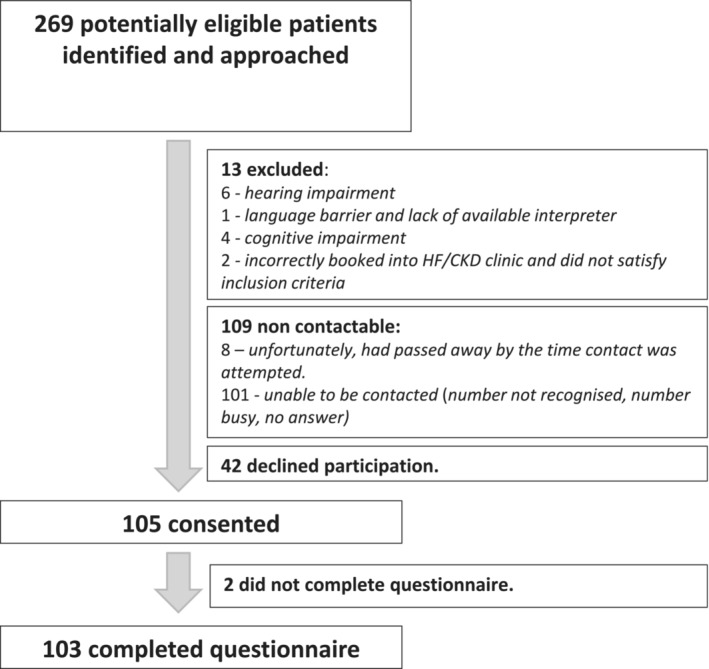
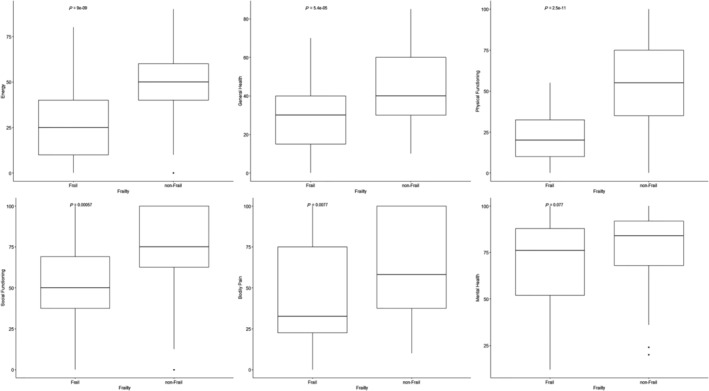
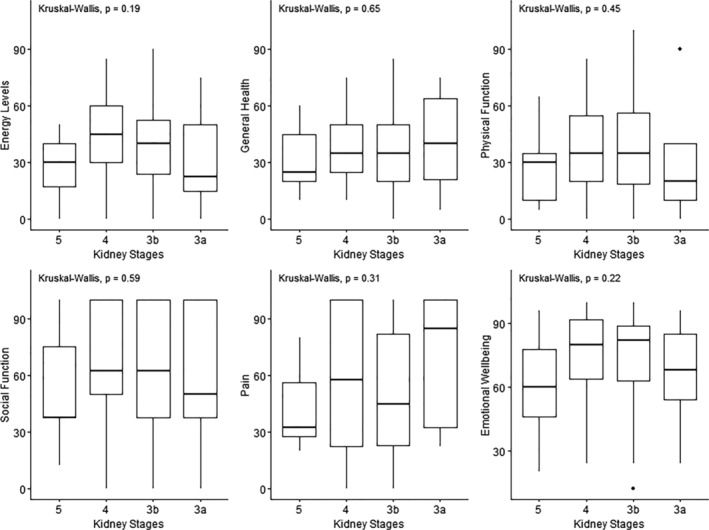
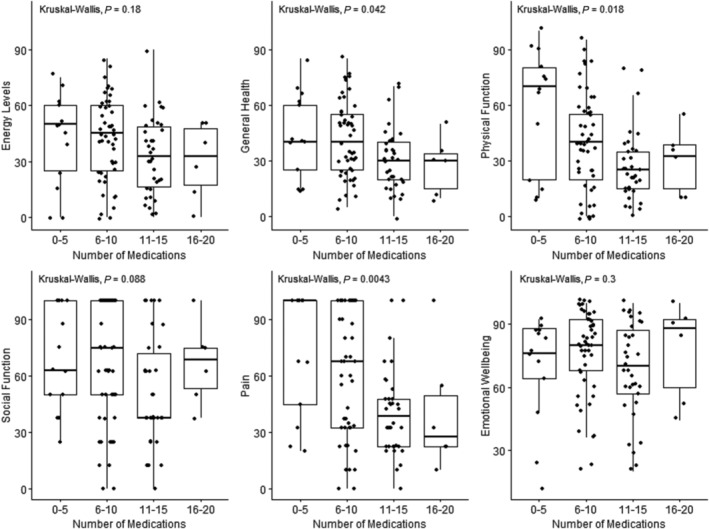
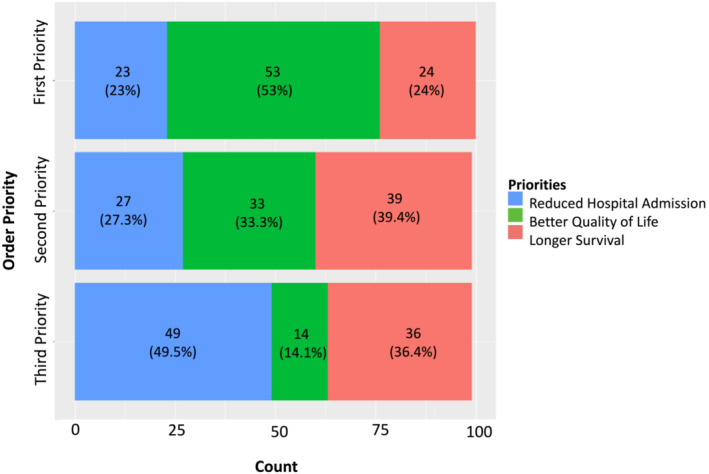
Methods and results: Patients were identified from a tertiary care cardiorenal clinic. Eligible patients had CKD-HF with a stable estimated glomerular filtration rate of <60 mL/min/1.732. Data were collected from each participant at one point in time using surveys delivered by study personnel between 14 July 2022 and 31 March 2023. Frailty was defined as Modified Frailty Phenotype (MFP) score ≥3. The Medical Outcomes Study 36-item Short Form Health Survey (SF-36) was used to assess QoL. Demographic data were retrospectively collected from electronic patient records. Demographics and QoL were compared between frail and non-frail cohorts using Pearson's R and Student's t-test (two-tailed, alpha-priori = 0.05). One hundred five participants consented, and 103 completed the questionnaires in full. Amongst the 103 participants, 49.5% (n = 51) were frail. Frailty was related to sex (P = 0.021) and medication count (P = 0.007), however not to other clinical measures, including estimated glomerular filtration rate (P = 0.437) and ejection fraction (P = 0.911). Frail patients reported poorer QoL across physical functioning (P < 0.001), general health (P < 0.001), bodily pain (P = 0.004), social functioning (P < 0.001), and energy levels (P < 0.001), however not emotional wellbeing (P = 0.058); 51.5% cited 'better quality of life' as their healthcare priority, over longer survival (23.3%) or avoiding hospital admissions (22.3%). This was consistent across frail and non-frail groups.
Conclusions: A large proportion of CKD-HF patients are frail, regardless of disease severity, and more susceptible to significantly poorer QoL across physical and social domains. Improving QoL is the priority of patients across both frail and non-frail cohorts, further emphasizing the need for prompt recognition of frailty as well as possible intervention and prevention.
Keywords: Chronic kidney failure; Frailty; Heart failure; Observational; Quality of life.
© 2024 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
The funding source had no role in study design, data collection, data analysis, data interpretation, or writing of the manuscript.
Figures
Similar articles
-
Frailty and quality of life: a cross-sectional study of Brazilian patients with pre-dialysis chronic kidney disease.Health Qual Life Outcomes. 2014 Feb 28;12:27. doi: 10.1186/1477-7525-12-27. Health Qual Life Outcomes. 2014. PMID: 24580960 Free PMC article.
-
Different impact of chronic kidney disease in older patients with heart failure according to frailty.Eur J Intern Med. 2025 Feb;132:90-96. doi: 10.1016/j.ejim.2024.12.001. Epub 2024 Dec 7. Eur J Intern Med. 2025. PMID: 39648049
-
Frailty Among Older Decompensated Heart Failure Patients: Prevalence, Association With Patient-Centered Outcomes, and Efficient Detection Methods.JACC Heart Fail. 2019 Dec;7(12):1079-1088. doi: 10.1016/j.jchf.2019.10.003. JACC Heart Fail. 2019. PMID: 31779931 Free PMC article.
-
[Frailty in renal diseases].Z Gerontol Geriatr. 2021 Nov;54(7):708-716. doi: 10.1007/s00391-021-01953-0. Epub 2021 Aug 5. Z Gerontol Geriatr. 2021. PMID: 34351485 Free PMC article. Review. German.
-
Multidomain Frailty in Heart Failure: Current Status and Future Perspectives.Curr Heart Fail Rep. 2021 Jun;18(3):107-120. doi: 10.1007/s11897-021-00513-2. Epub 2021 Apr 9. Curr Heart Fail Rep. 2021. PMID: 33835397 Review.
Cited by
-
Investigating frailty and quality of life in patients with heart failure and CKD (FRAIL study).ESC Heart Fail. 2025 Feb;12(1):5-7. doi: 10.1002/ehf2.15096. Epub 2024 Sep 19. ESC Heart Fail. 2025. PMID: 39295500 Free PMC article. No abstract available.
-
Burden of heart failure attributable to chronic kidney disease in older adults (1990-2021): an analysis from the global burden of disease study.Front Public Health. 2025 Jun 18;13:1606719. doi: 10.3389/fpubh.2025.1606719. eCollection 2025. Front Public Health. 2025. PMID: 40606121 Free PMC article.
-
Baseline Characteristics of Frailty and Disease Stage in Older People Living With CKD.Kidney Int Rep. 2024 Oct 15;10(1):120-133. doi: 10.1016/j.ekir.2024.10.009. eCollection 2025 Jan. Kidney Int Rep. 2024. PMID: 39810773 Free PMC article.
-
Exercise for frailty research frontiers: a bibliometric analysis and systematic review.Front Med (Lausanne). 2024 May 1;11:1341336. doi: 10.3389/fmed.2024.1341336. eCollection 2024. Front Med (Lausanne). 2024. PMID: 38751977 Free PMC article.
-
Domiciliary subcutaneous furosemide in patients with CKD and HF: a quality improvement project.BMJ Open Qual. 2025 Apr 10;14(2):e002984. doi: 10.1136/bmjoq-2024-002984. BMJ Open Qual. 2025. PMID: 40216456 Free PMC article.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
