

MYC targeting by OMO-103 in solid tumors: a phase 1 trial
- PMID: 38321218
- PMCID: PMC10957469
- DOI: 10.1038/s41591-024-02805-1
MYC targeting by OMO-103 in solid tumors: a phase 1 trial
Abstract
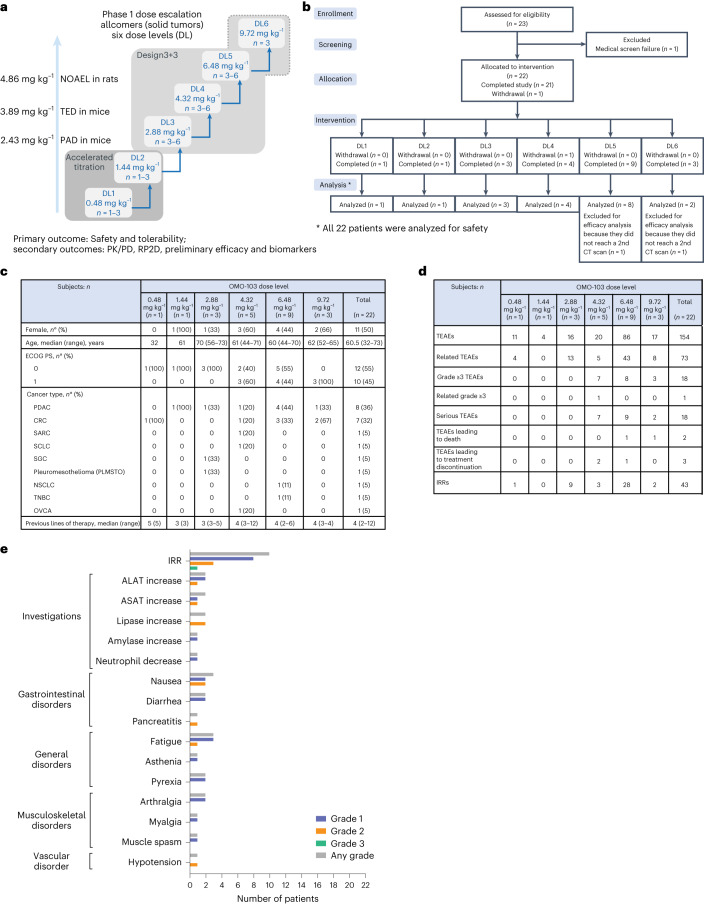
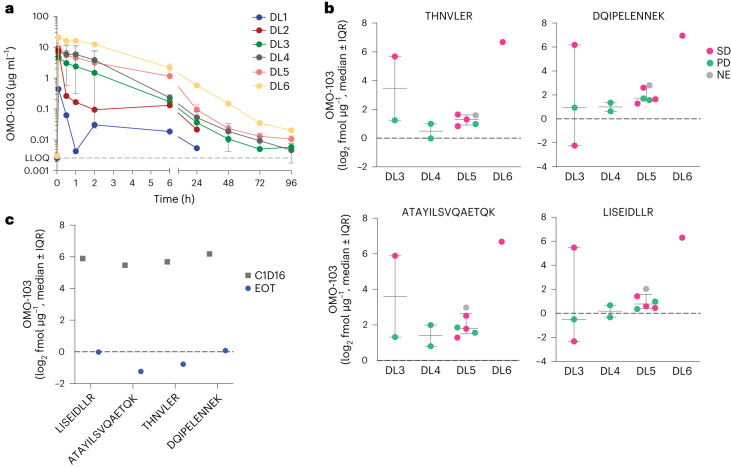
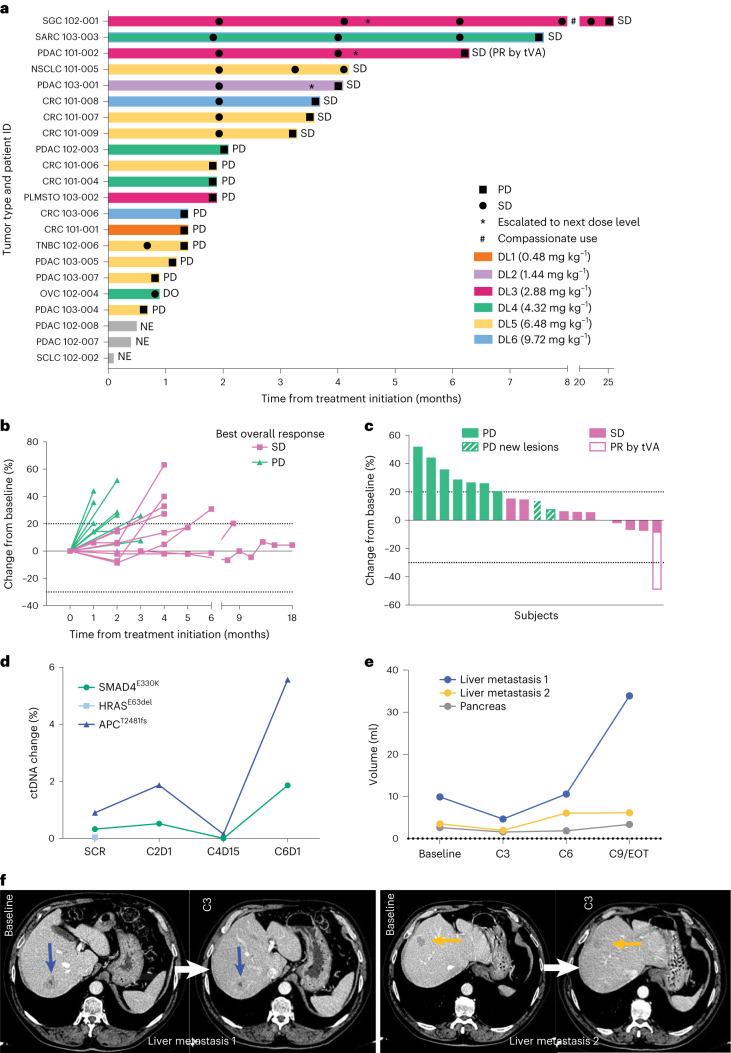
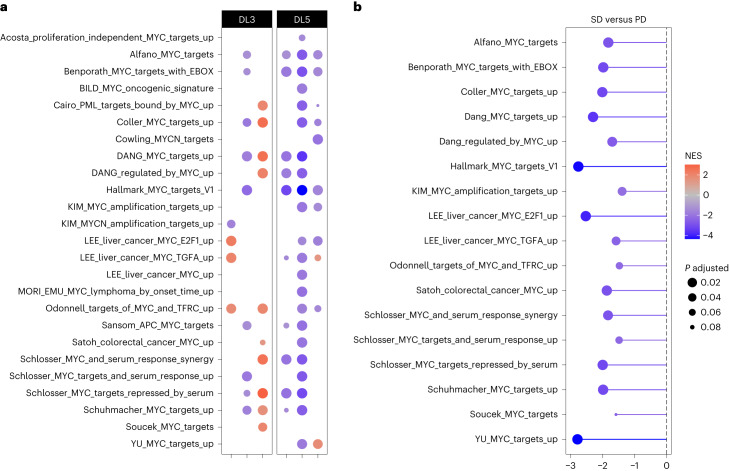
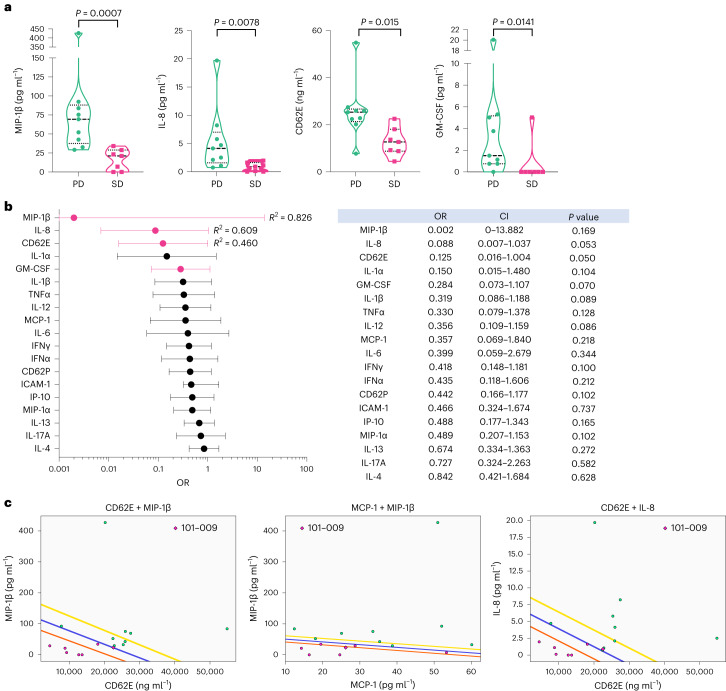
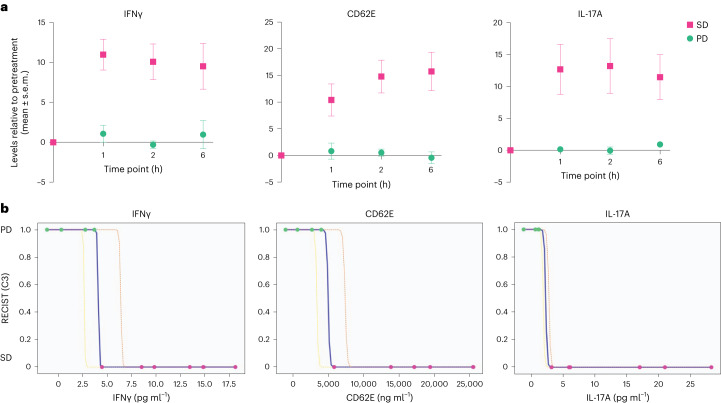
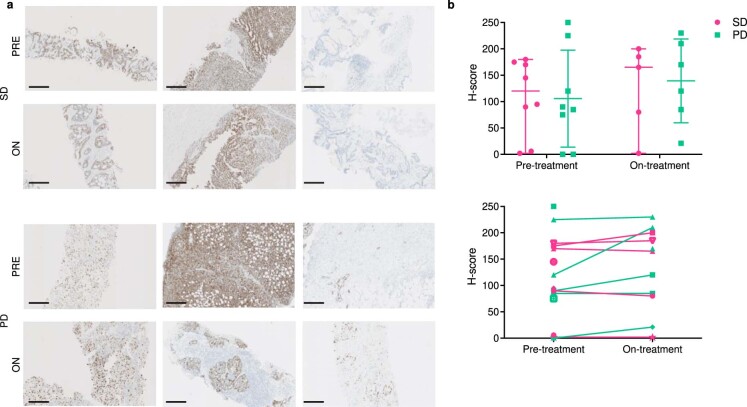
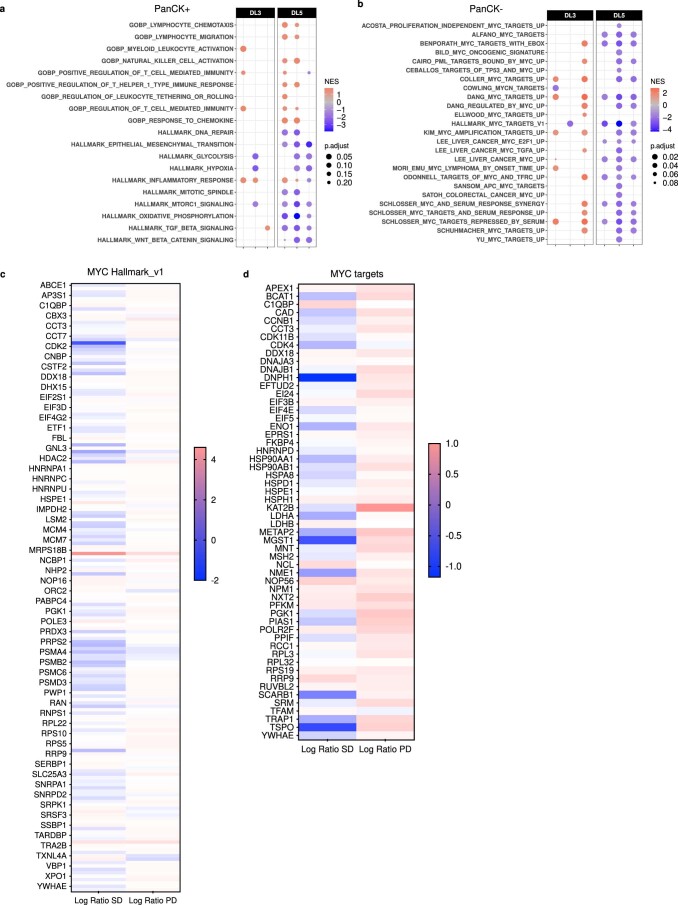
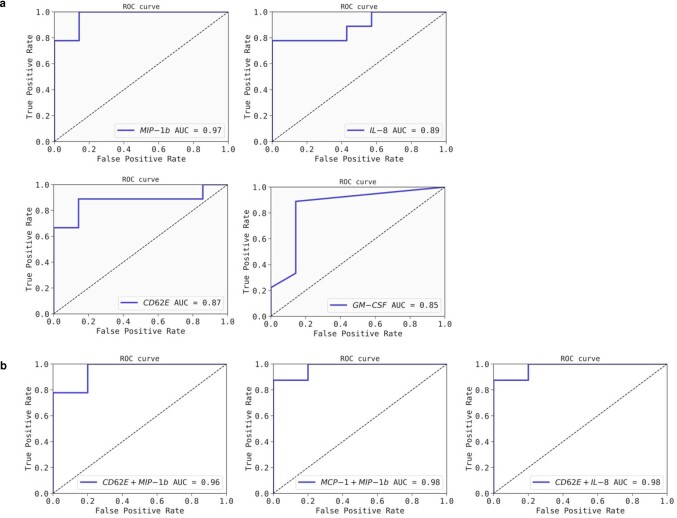
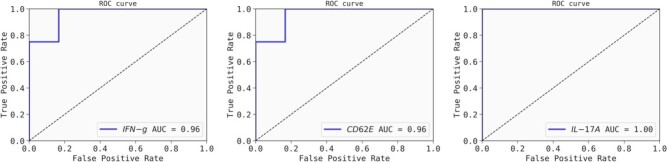
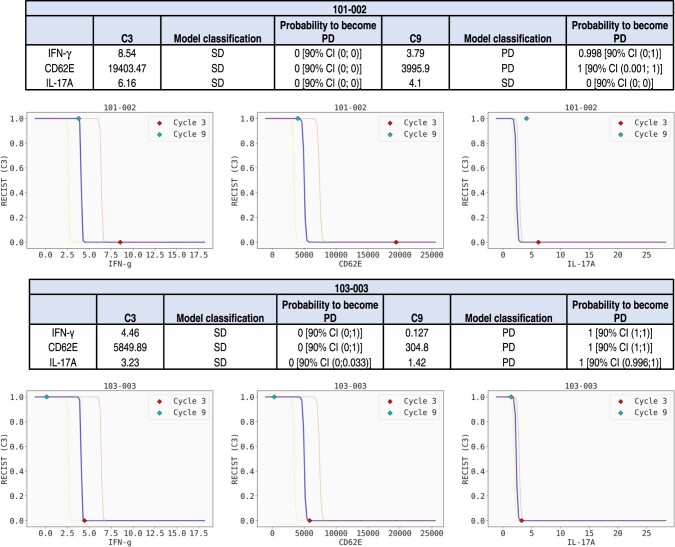
Among the 'most wanted' targets in cancer therapy is the oncogene MYC, which coordinates key transcriptional programs in tumor development and maintenance. It has, however, long been considered undruggable. OMO-103 is a MYC inhibitor consisting of a 91-amino acid miniprotein. Here we present results from a phase 1 study of OMO-103 in advanced solid tumors, established to examine safety and tolerability as primary outcomes and pharmacokinetics, recommended phase 2 dose and preliminary signs of activity as secondary ones. A classical 3 + 3 design was used for dose escalation of weekly intravenous, single-agent OMO-103 administration in 21-day cycles, encompassing six dose levels (DLs). A total of 22 patients were enrolled, with treatment maintained until disease progression. The most common adverse events were grade 1 infusion-related reactions, occurring in ten patients. One dose-limiting toxicity occurred at DL5. Pharmacokinetics showed nonlinearity, with tissue saturation signs at DL5 and a terminal half-life in serum of 40 h. Of the 19 patients evaluable for response, 12 reached the predefined 9-week time point for assessment of drug antitumor activity, eight of those showing stable disease by computed tomography. One patient defined as stable disease by response evaluation criteria in solid tumors showed a 49% reduction in total tumor volume at best response. Transcriptomic analysis supported target engagement in tumor biopsies. In addition, we identified soluble factors that are potential pharmacodynamic and predictive response markers. Based on all these data, the recommended phase 2 dose was determined as DL5 (6.48 mg kg-1).ClinicalTrials.gov identifier: NCT04808362 .
© 2024. The Author(s).
Conflict of interest statement
E.G. is Consultant-Advisor for Roche/Genentech, F.Hoffmann/La Roche, Ellipses Pharma, Neomed Therapeutics1, Inc., Boehringer Ingelheim, Janssen Global Services, SeaGen, TFS, Alkermes, Thermo Fisher, Bristol-Myers Squibb, MabDiscovery, Anaveon, F-Star Therapeutics and Hengrui. L.S. is Consultant and CEO of Peptomyc. V.M. is Consultant of Roche, Bayer, BMS, Janssen and Basilea. E.C. is Consultant-Advisor for Nanobiotix, Janssen-Cilag, Roche-Genentech, TargImmune Therapeutics, Servier, Bristol-Myers Squibb, Amunix, Adcendo, Anaveon, AstraZeneca/Medimmune, Chugai Pharma, MonTa, MSD Oncology, Nouscom, OncoDNA, T-Knife, Elevation Oncology, PharmaMar, Ellipses Pharma, Syneos Health, Genmab and Diaccurate. Employment. M.-E.B., S.C.-S., S.M.-M., L.F., S.L.-E., V.C.C., J.M., M.N. and L.S. are employees of Peptomyc. E.C. is an employee of START. Personal financial interests: L.S. and M.-E.B. are cofounders and shareholders of Peptomyc and inventors of patent application no. WO2014180889 A8 that covers the use of the Omomyc miniprotein in medicine, held by VHIO and licenced to Peptomyc. S.C.-S., S.L.-E., L.F., J.R.W. and M.N. are also shareholders of Peptomyc. E.G. performs research for Novartis, Roche, Thermo Fisher, AstraZeneca, Taiho and BeiGene; she is in Speakers Bureau for Merck Sharp & Dohme, Roche, Thermo Fisher, Lilly and Novartis; she runs clinical trials as PI or Co-PI with Agios Pharmaceuticals, Amgen, Bayer, Beigene USA, Blueprint Medicines, BMS, Cellestia Biotech, Debiopharm, F.Hoffmann/La Roche, Ltd, Forma Therapeutics, Genentech, Inc., Genmab B.V., GSK, Glycotope Gmbh, Incyte Biosciences, Incyte Corporation, ICO, Kura Oncology, Inc, Lilly, S.A, Loxo Oncology, Inc, Macrogenics, Inc, Menarini Ricerche Spa, Merck, Sharp & Dohme de España, S.A, Nanobiotix, S.A, Novartis Farmacéutica, S.A, Pfizer, SLU, Pharma Mar, S.A.U, Pierre Fabre Medicament, Principia Biopharma, Inc., Psioxus Therapeutics, Ltd, Sanofi, Sierra Oncology, Inc, Sotio A.S and Symphogen A/S. V.M. is Principal Investigator and receives institutional funding from AbbVie, AceaBio, Adaptimmune, ADC Therapeutics, Aduro, Agenus, Amcure, Amgen, Astellas, AstraZeneca Bayer Beigene BioInvent International AB, BMS, Boehringer, Boheringer, Boston, Celgene, Daichii Sankyo, DEBIOPHARM, Eisai, e-Terapeutics, Exelisis, Forma Therapeutics, Genmab, GSK, Harpoon, Hutchison, Immutep, Incyte, Inovio, Iovance, Janssen, Kyowa Kirin, Lilly, Loxo, MedSir, Menarini, Merck, Merus, Millennium, MSD, Nanobiotix, Nektar, Novartis, Odonate Therapeutics, Pfizer, Pharma Mar, PharmaMar, Principia, PsiOxus, Puma, Regeneron, Rigontec, Roche, Sanofi, Sierra Oncology, Synthon, Taiho, Takeda, Tesaro, Transgene, Turning Point Therapeutics and Upshersmith. E.C. is Principal Investigator and receives institutional funding from START, Pharma Mar, EORTC, Sanofi, BeiGene, Novartis and Merus N.V.; he is a shareholder of START and Oncoart Associated and receives honoraria from HM Hospitales Group; he receives research funding from START; he is President and Founder of Foundation Investigational Therapeutics in Oncological Sciences; and he has a not-for-profit relationship with PharmaMar and the CRIS Cancer Foundation. The other authors declare no competing interests.
Figures
Comment in
-
MYC inhibitor achieves phase I success.Nat Rev Drug Discov. 2024 Apr;23(4):253. doi: 10.1038/d41573-024-00042-2. Nat Rev Drug Discov. 2024. PMID: 38448668 No abstract available.
References
-
- Stine ZE, Walton ZE, Altman BJ, Hsieh AL, Dang CV. MYC, metabolism, and cancer. Cancer Discov. 2015;5:1024–1039. doi: 10.1158/2159-8290.CD-15-0507. - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
- 872212/EC | EU Framework Programme for Research and Innovation H2020 | H2020 Priority Excellent Science | H2020 Research Infrastructures (H2020 Excellent Science - Research Infrastructures)
- 872212/EC | EU Framework Programme for Research and Innovation H2020 | H2020 Excellent Science (H2020 Priority Excellent Science)
LinkOut - more resources
Full Text Sources
Medical
