

Assessing Symptomatic Hypocalcemia Risk After Total Thyroidectomy: A Prospective Study
- PMID: 38322433
- PMCID: PMC10843930
- DOI: 10.1055/s-0043-1777450
Assessing Symptomatic Hypocalcemia Risk After Total Thyroidectomy: A Prospective Study
Abstract
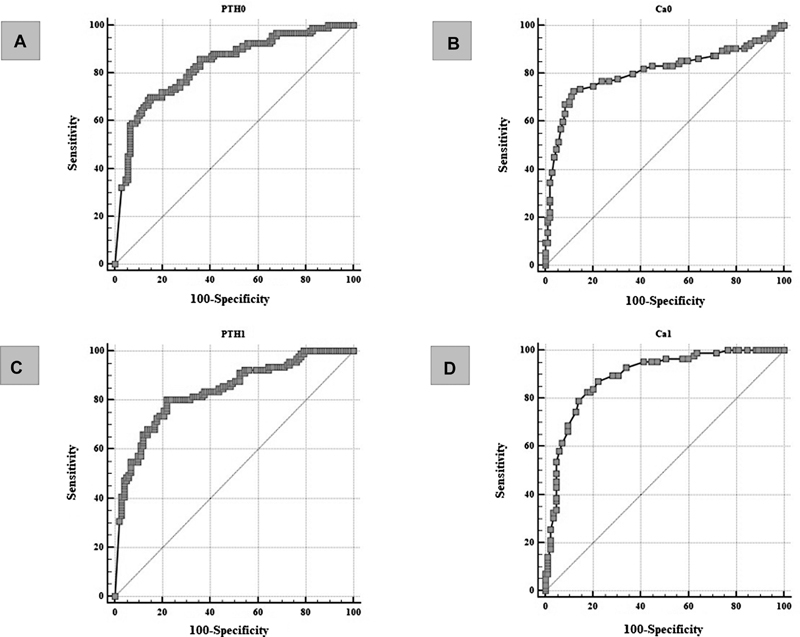
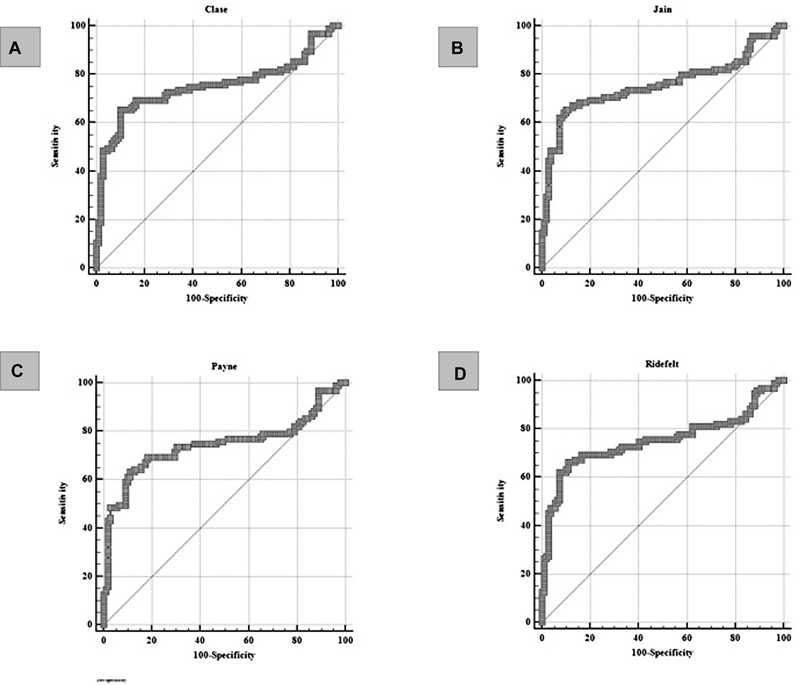
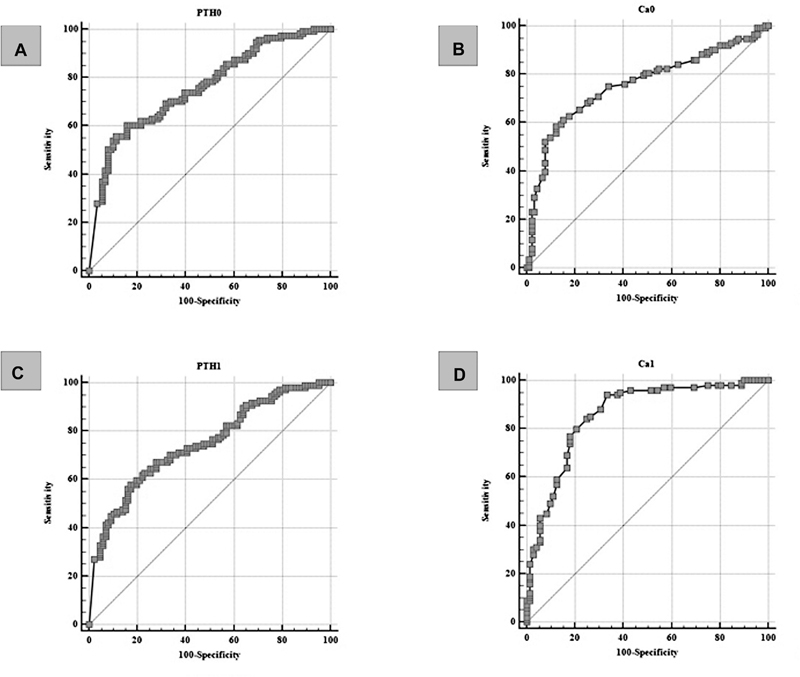
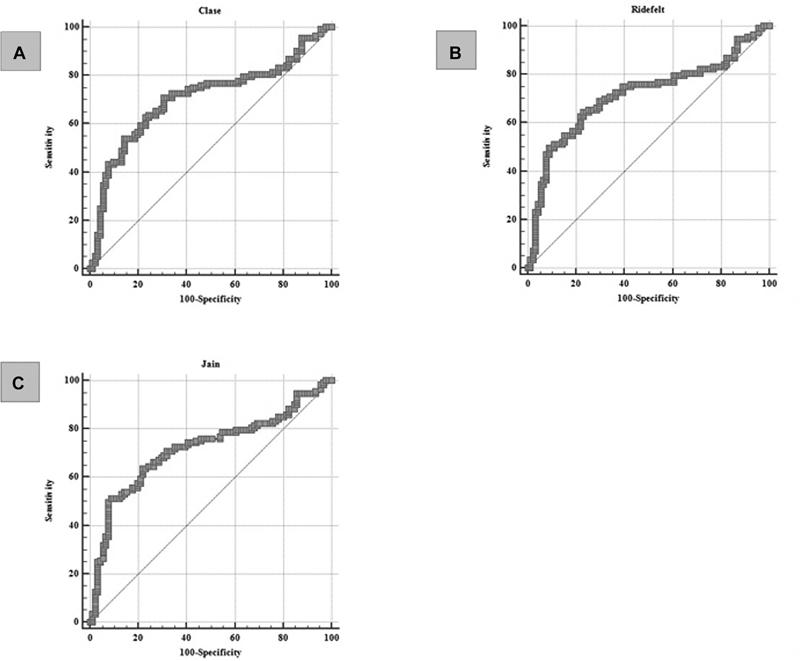
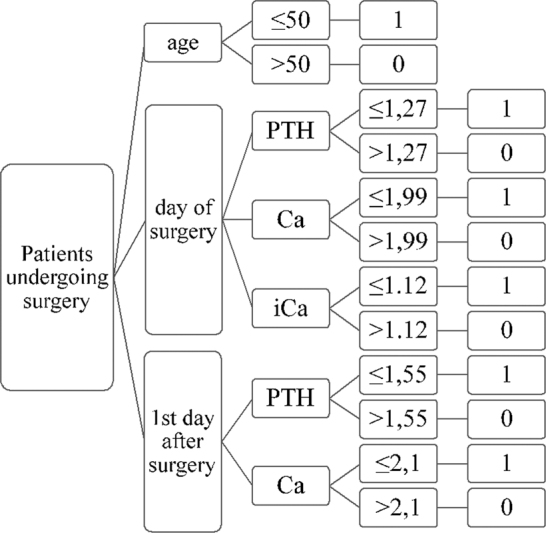
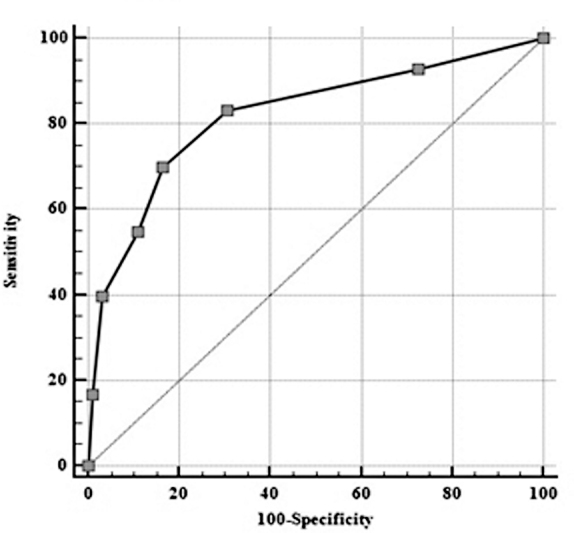
Introduction The most common postoperative complication of total thyroidectomy is hypocalcemia, usually monitored using serum parathyroid hormone and calcium values. Objective To identify the most accurate predictors of hypocalcemia, construct a risk assesment algorithm and analyze the impact of using several calcium correction formulas in practice. Methods A prospective, single-center, non-randomized longitudinal cohort study on 205 patients undergoing total thyroidectomy. Parathyroid hormone, serum, and ionized calcium were sampled post-surgery, with the presence of symptomatic or laboratory-verified asymptomatic hypocalcemia designated as primary outcome measures. Results Parathyroid hormone sampled on the first postoperative day was the most sensitive predictor of symptomatic hypocalcemia development (sensitivity 80.22%, cut-off value ≤2.03 pmol/L). A combination of serum calcium and parathyroid concentration sampled on the first postoperative day predicted the development of hypocalcemia during recovery with the highest sensitivity and specificity (94% sensitivity, cut-off ≤2.1 mmol/L, and 89% specificity, cut-off ≤1.55 pmol/L, respectively). The use of algorithms and correction formulas did not improve the accuracy of predicting symptomatic or asymptomatic hypocalcemia. Conclusions The most sensitive predictor of symptomatic hypocalcemia present on the fifth postoperative day was PTH sampled on the first postoperative day. The need for algorithms and correction formulas is limited.
Keywords: calcium; hypocalcemia; parathyroid hormone; risk assessment; total thyroidectomy.
The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution 4.0 International License, permitting copying and reproduction so long as the original work is given appropriate credit ( https://creativecommons.org/licenses/by/4.0/ ).
Figures
Similar articles
-
Identifying early postoperative serum parathyroid hormone levels as predictors of hypocalcaemia after total thyroidectomy: A prospective non-randomized study.Am J Otolaryngol. 2020 May-Jun;41(3):102416. doi: 10.1016/j.amjoto.2020.102416. Epub 2020 Feb 4. Am J Otolaryngol. 2020. PMID: 32046865 Clinical Trial.
-
Postoperative Serum Parathyroid Hormone Levels as a Predictor of Hypocalcemia in Patients Undergoing Total Thyroidectomy.Indian J Otolaryngol Head Neck Surg. 2023 Jun;75(2):255-260. doi: 10.1007/s12070-022-03172-4. Epub 2022 Oct 8. Indian J Otolaryngol Head Neck Surg. 2023. PMID: 37275104 Free PMC article.
-
Prospective evaluation of intra-operative quick parathyroid hormone assay as an early predictor of post thyroidectomy hypocalcaemia.Int J Surg. 2016 Oct;34:103-108. doi: 10.1016/j.ijsu.2016.08.010. Epub 2016 Aug 12. Int J Surg. 2016. PMID: 27530498
-
Risk factors for the development of hypocalcemia in pediatric patients after total thyroidectomy - A systematic review.Int J Pediatr Otorhinolaryngol. 2021 Apr;143:110666. doi: 10.1016/j.ijporl.2021.110666. Epub 2021 Mar 4. Int J Pediatr Otorhinolaryngol. 2021. PMID: 33706109
-
The role and timing of parathyroid hormone determination after total thyroidectomy.Gland Surg. 2017 Dec;6(Suppl 1):S38-S48. doi: 10.21037/gs.2017.09.06. Gland Surg. 2017. PMID: 29322021 Free PMC article. Review.
Cited by
-
Hypocalcemia Following Thyroidectomy in a Patient With COVID-19: A Case Report and Literature Review.Cureus. 2024 Aug 12;16(8):e66665. doi: 10.7759/cureus.66665. eCollection 2024 Aug. Cureus. 2024. PMID: 39262524 Free PMC article.
-
The evolution and clinical impact of single-port transaxillary robotic thyroidectomy: a comprehensive review.Gland Surg. 2025 Jan 24;14(1):74-81. doi: 10.21037/gs-24-409. Epub 2025 Jan 9. Gland Surg. 2025. PMID: 39958894 Free PMC article. Review.
References
-
- Papavramidis T S, Anastasiou O, Pliakos I, Kotsovolis G, Panidis S, Michalopoulos A. Parathyroid function after total thyroidectomy: A randomized clinical trial concerning the influence of the surgical technique. Endocr Pract. 2018;24(02):150–155. - PubMed
-
- Bashir A Y, Alzubaidi A N, Bashir M A et al.The Optimal Parathyroid Hormone Cut-Off Threshold for Early and Safe Management of Hypocalcemia After Total Thyroidectomy. Endocr Pract. 2021;27(09):925–933. - PubMed
LinkOut - more resources
Full Text Sources