

Could an integrated model of health and social care after critical illness reduce socioeconomic disparities in outcomes? A Bayesian analysis
- PMID: 38322488
- PMCID: PMC10844938
- DOI: 10.1016/j.bjao.2024.100259
Could an integrated model of health and social care after critical illness reduce socioeconomic disparities in outcomes? A Bayesian analysis
Abstract
Background: There is limited evidence to understand what impact, if any, recovery services might have for patients across the socioeconomic spectrum after critical illness. We analysed data from a multicentre critical care recovery programme to understand the impact of this programme across the socioeconomic spectrum.
Methods: The setting for this pre-planned secondary analysis was a critical care rehabilitation programme-Intensive Care Syndrome: Promoting Independence and Return to Employment. Data were collected from five hospital sites running this programme. We utilised a Bayesian approach to analysis and explore any possible effect of the InS:PIRE intervention on Health-Related Quality of Life (HRQoL) across the socioeconomic gradient. A Bayesian quantile, non-linear mixed effects regression model, using a compound symmetry covariance structure, accounting for multiple timepoints was utilised. The Scottish Index of Multiple Deprivation (SIMD) was used to measure socioeconomic status and HRQoL was measured using the EQ-5D-5L.
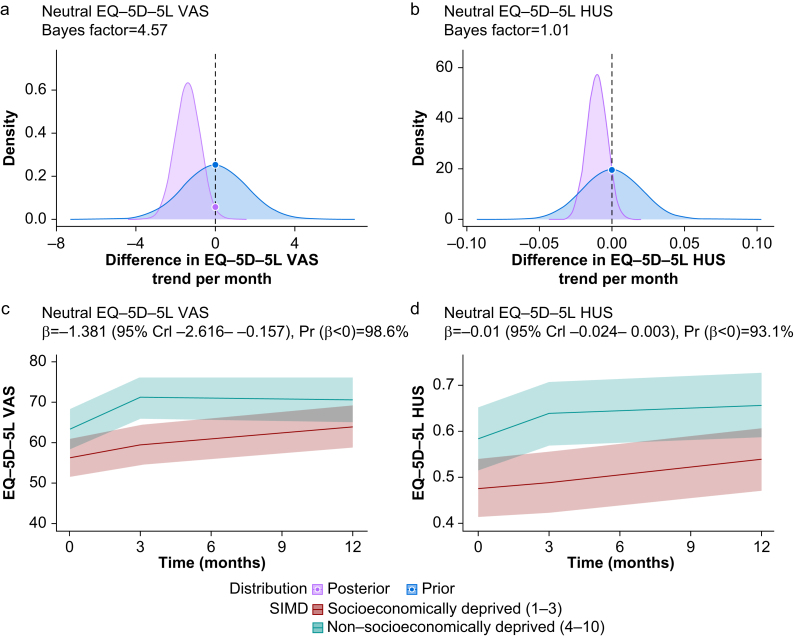
Results: In the initial baseline cohort of 182 patients, 55% of patients were male, the median age was 58 yr (inter-quartile range: 50-66 yr) and 129 (79%) patients had two or more comorbidities at ICU admission. Using the neutral prior, there was an overall probability of intervention benefit of 100% (β=0.71, 95% credible interval: 0.34-1.09) over 12 months to those in the SIMD≤3 cohort, and an 98.6% (β=-1.38, 95% credible interval: -2.62 to -0.16) probability of greater benefit (i.e. a steeper increase in improvement) at 12 months in the SIMD≤3 vs SIMD≥4 cohort in the EQ-visual analogue scale.
Conclusions: Using multicentre data, this re-analysis suggests, but does not prove, that an integrated health and social care intervention is likely to improve outcomes across the socioeconomic gradient after critical illness, with a potentially greater benefit for those from deprived communities. Future research designed to prospectively analyse how critical care recovery programmes could potentially improve outcomes across the socioeconomic gradient is warranted.
Keywords: Bayesian; critical illness; deprivation; quality of life; socioeconomic.
© 2024 The Authors.
Figures
Similar articles
-
Evaluation of a health and social care programme to improve outcomes following critical illness: a multicentre study.Thorax. 2023 Feb;78(2):160-168. doi: 10.1136/thoraxjnl-2021-218428. Epub 2022 Mar 21. Thorax. 2023. PMID: 35314485 Free PMC article.
-
Intensive Care Syndrome: Promoting Independence and Return to Employment (InS:PIRE). Early evaluation of a complex intervention.PLoS One. 2017 Nov 29;12(11):e0188028. doi: 10.1371/journal.pone.0188028. eCollection 2017. PLoS One. 2017. PMID: 29186177 Free PMC article.
-
Socioeconomic deprivation and illness trajectory in the Scottish population after COVID-19 hospitalization.Commun Med (Lond). 2024 Feb 28;4(1):32. doi: 10.1038/s43856-024-00455-5. Commun Med (Lond). 2024. PMID: 38418616 Free PMC article.
-
Impact of a social prescribing intervention in North East England on adults with type 2 diabetes: the SPRING_NE multimethod study.Public Health Res (Southampt). 2023 Mar;11(2):1-185. doi: 10.3310/AQXC8219. Public Health Res (Southampt). 2023. PMID: 37254700
-
Systematic reviews of the effectiveness of day care for people with severe mental disorders: (1) acute day hospital versus admission; (2) vocational rehabilitation; (3) day hospital versus outpatient care.Health Technol Assess. 2001;5(21):1-75. doi: 10.3310/hta5210. Health Technol Assess. 2001. PMID: 11532238 Review.
Cited by
-
Exploring the Landscape of Social and Economic Factors in Critical Illness Survivorship: A Scoping Review.Crit Care Explor. 2025 Feb 7;7(2):e1208. doi: 10.1097/CCE.0000000000001208. eCollection 2025 Feb 1. Crit Care Explor. 2025. PMID: 39919212 Free PMC article.
-
Relationship between critical illness recovery and social determinants of health: a multiperspective qualitative study in British Columbia, Canada.BMJ Open. 2024 Nov 19;14(11):e089086. doi: 10.1136/bmjopen-2024-089086. BMJ Open. 2024. PMID: 39566939 Free PMC article.
References
-
- Mikkelsen M.E., Still M., Anderson B.J., et al. Society of critical care medicine's international consensus conference on prediction and identification of long-term impairments after critical illness. Crit Care Med. 2020;48:1670–1679. - PubMed
-
- McPeake J., Mikkelsen M.E., Quasim T., et al. Return to employment after critical illness and its association with psychosocial outcomes. A systematic review and meta-analysis. Ann Am Thorac Soc. 2019;16:1304–1311. - PubMed
-
- McPeake J., Bateson M., Christie F., et al. Hospital re-admission after critical care survival: a systematic review and meta-analysis. Anaesthesia. 2022;77:475–485. - PubMed
LinkOut - more resources
Full Text Sources
