

Comprehensive Analysis of a Japanese Pedigree with Biallelic ACAGG Expansions in RFC1 Manifesting Motor Neuronopathy with Painful Muscle Cramps
- PMID: 38324175
- PMCID: PMC11269323
- DOI: 10.1007/s12311-024-01666-1
Comprehensive Analysis of a Japanese Pedigree with Biallelic ACAGG Expansions in RFC1 Manifesting Motor Neuronopathy with Painful Muscle Cramps
Abstract
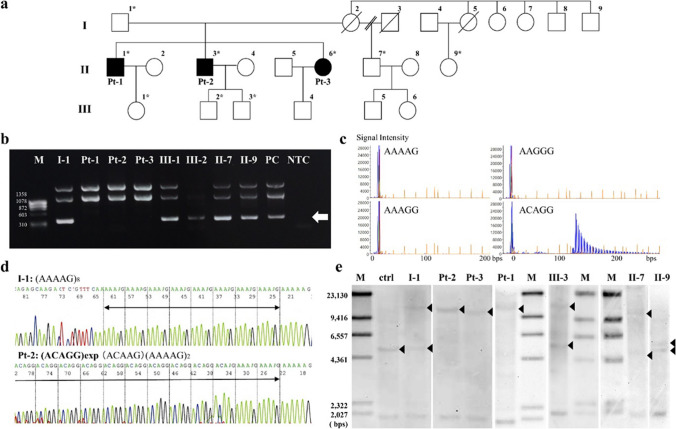
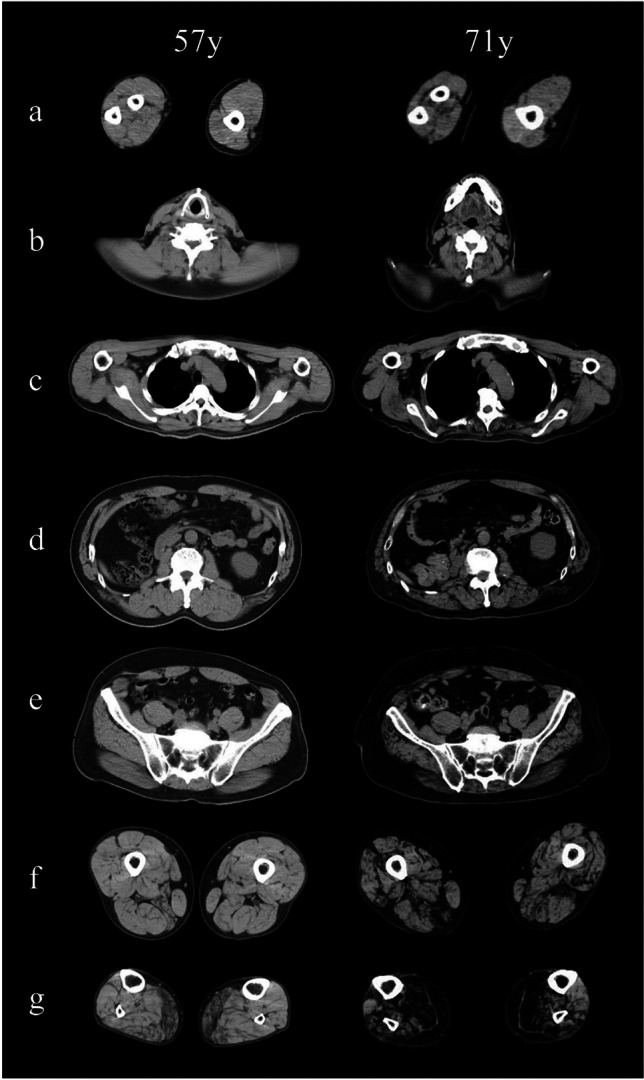
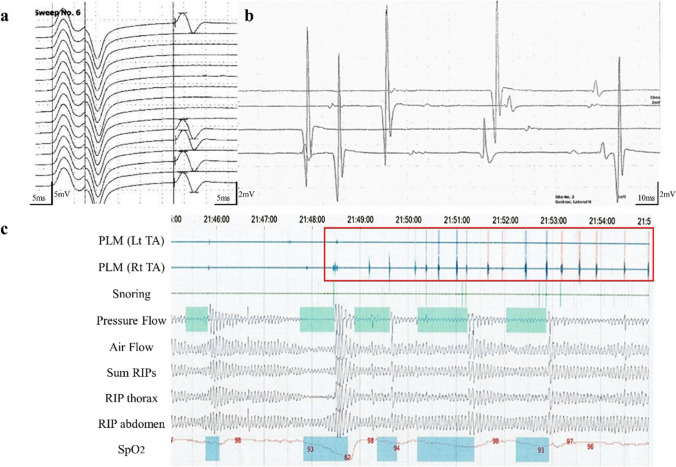
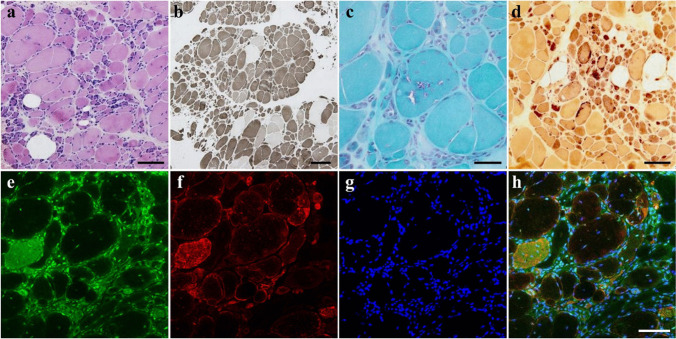
Cerebellar ataxia, neuropathy, and vestibular areflexia syndrome (CANVAS) is an autosomal recessive multisystem neurologic disorder caused by biallelic intronic repeats in RFC1. Although the phenotype of CANVAS has been expanding via diagnostic case accumulation, there are scant pedigree analyses to reveal disease penetrance, intergenerational fluctuations in repeat length, or clinical phenomena (including heterozygous carriers). We identified biallelic RFC1 ACAGG expansions of 1000 ~ repeats in three affected siblings having sensorimotor neuronopathy with spinocerebellar atrophy initially presenting with painful muscle cramps and paroxysmal dry cough. They exhibit almost homogeneous clinical and histopathological features, indicating motor neuronopathy. Over 10 years of follow-up, painful intractable muscle cramps ascended from legs to trunks and hands, followed by amyotrophy and subsequent leg pyramidal signs. The disease course combined with the electrophysical and imagery data suggest initial and prolonged hyperexcitability and the ensuing spinal motor neuron loss, which may progress from the lumbar to the rostral anterior horns and later expand to the corticospinal tract. Genetically, heterozygous ACAGG expansions of similar length were transmitted in unaffected family members of three successive generations, and some of them experienced muscle cramps. Leukocyte telomere length assays revealed comparatively shorter telomeres in affected individuals. This comprehensive pedigree analysis demonstrated a non-anticipating ACAGG transmission and high penetrance of manifestations with a biallelic state, especially motor neuronopathy in which muscle cramps serve as a prodromal and disease progress marker. CANVAS and RFC1 spectrum disorder should be considered when diagnosing lower dominant motor neuron disease, idiopathic muscle cramps, or neuromuscular hyperexcitability syndromes.
Keywords: RFC1; ACAGG; CANVAS; Motor neuronopathy; Muscle cramp; Telomere.
© 2024. The Author(s).
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
References
-
- Malaquias MJ, Braz L, Santos Silva C, Damasio J, Jorge A, Lemos JM, et al. Multisystemic RFC1-related disorder: expanding the phenotype beyond cerebellar ataxia, neuropathy, and vestibular areflexia syndrome. Neurol Clin Pract. 2023;13:e200190. 10.1212/CPJ.0000000000200190. 10.1212/CPJ.0000000000200190 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
