

Time to Treatment With Intravenous Thrombolysis Before Thrombectomy and Functional Outcomes in Acute Ischemic Stroke: A Meta-Analysis
- PMID: 38324409
- PMCID: PMC10851137
- DOI: 10.1001/jama.2024.0589
Time to Treatment With Intravenous Thrombolysis Before Thrombectomy and Functional Outcomes in Acute Ischemic Stroke: A Meta-Analysis
Abstract
Importance: The benefit of intravenous thrombolysis (IVT) for acute ischemic stroke declines with longer time from symptom onset, but it is not known whether a similar time dependency exists for IVT followed by thrombectomy.
Objective: To determine whether the benefit associated with IVT plus thrombectomy vs thrombectomy alone decreases with treatment time from symptom onset.
Design, setting, and participants: Individual participant data meta-analysis from 6 randomized clinical trials comparing IVT plus thrombectomy vs thrombectomy alone. Enrollment was between January 2017 and July 2021 at 190 sites in 15 countries. All participants were eligible for IVT and thrombectomy and presented directly at thrombectomy-capable stroke centers (n = 2334). For this meta-analysis, only patients with an anterior circulation large-vessel occlusion were included (n = 2313).
Exposure: Interval from stroke symptom onset to expected administration of IVT and treatment with IVT plus thrombectomy vs thrombectomy alone.
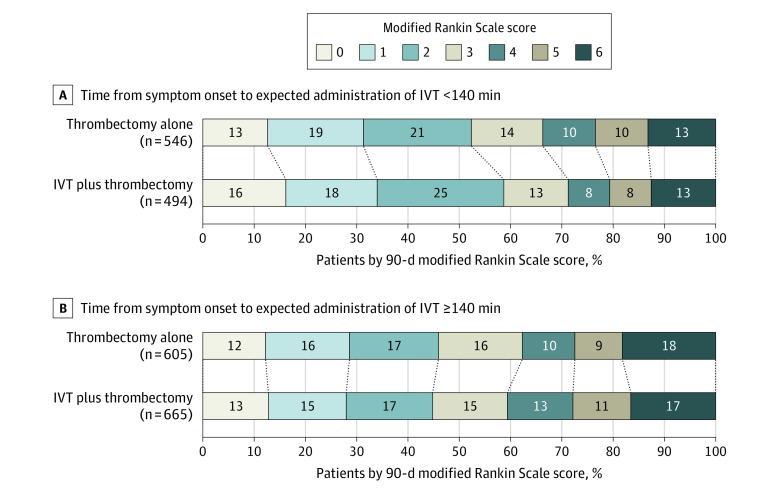
Main outcomes and measures: The primary outcome analysis tested whether the association between the allocated treatment (IVT plus thrombectomy vs thrombectomy alone) and disability at 90 days (7-level modified Rankin Scale [mRS] score range, 0 [no symptoms] to 6 [death]; minimal clinically important difference for the rates of mRS scores of 0-2: 1.3%) varied with times from symptom onset to expected administration of IVT.
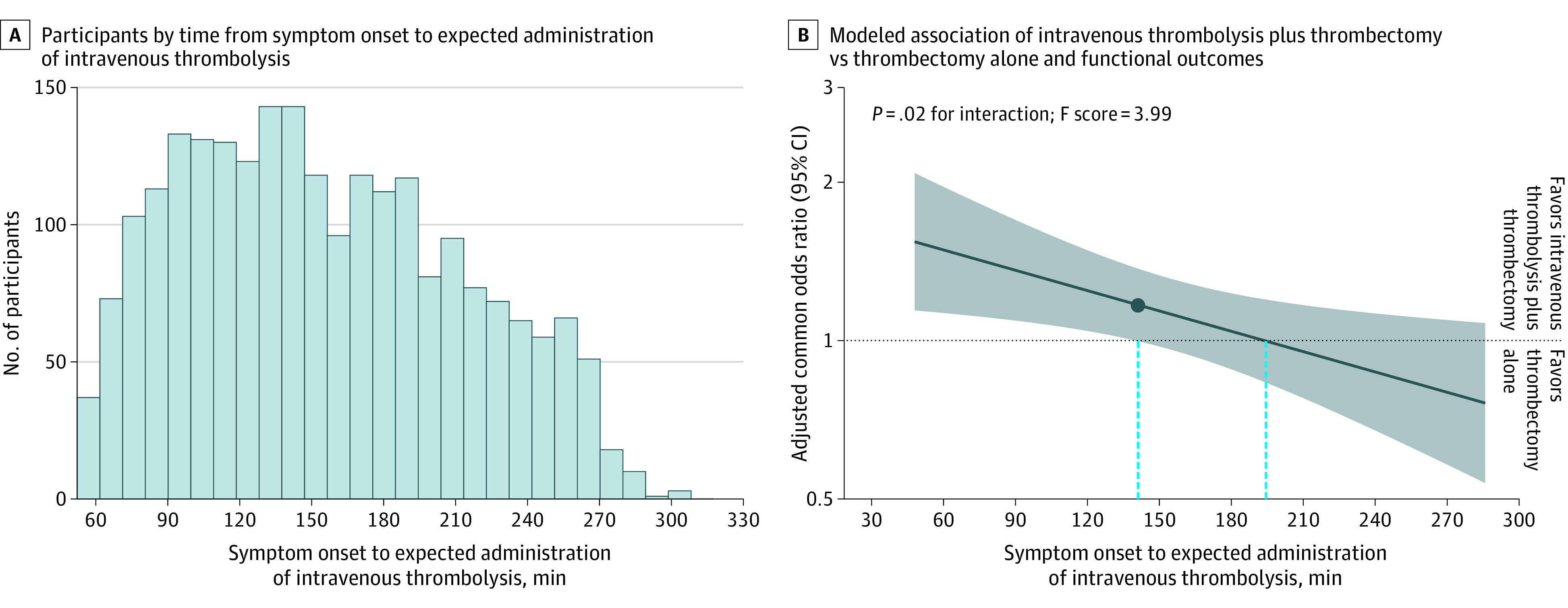
Results: In 2313 participants (1160 in IVT plus thrombectomy group vs 1153 in thrombectomy alone group; median age, 71 [IQR, 62 to 78] years; 44.3% were female), the median time from symptom onset to expected administration of IVT was 2 hours 28 minutes (IQR, 1 hour 46 minutes to 3 hours 17 minutes). There was a statistically significant interaction between the time from symptom onset to expected administration of IVT and the association of allocated treatment with functional outcomes (ratio of adjusted common odds ratio [OR] per 1-hour delay, 0.84 [95% CI, 0.72 to 0.97], P = .02 for interaction). The benefit of IVT plus thrombectomy decreased with longer times from symptom onset to expected administration of IVT (adjusted common OR for a 1-step mRS score shift toward improvement, 1.49 [95% CI, 1.13 to 1.96] at 1 hour, 1.25 [95% CI, 1.04 to 1.49] at 2 hours, and 1.04 [95% CI, 0.88 to 1.23] at 3 hours). For a mRS score of 0, 1, or 2, the predicted absolute risk difference was 9% (95% CI, 3% to 16%) at 1 hour, 5% (95% CI, 1% to 9%) at 2 hours, and 1% (95% CI, -3% to 5%) at 3 hours. After 2 hours 20 minutes, the benefit associated with IVT plus thrombectomy was not statistically significant and the point estimate crossed the null association at 3 hours 14 minutes.
Conclusions and relevance: In patients presenting at thrombectomy-capable stroke centers, the benefit associated with IVT plus thrombectomy vs thrombectomy alone was time dependent and statistically significant only if the time from symptom onset to expected administration of IVT was short.
Conflict of interest statement
Figures
Comment in
-
Time to IVT Treatment and Functional Outcomes in Acute Ischemic Stroke.JAMA. 2024 Jun 18;331(23):2048-2049. doi: 10.1001/jama.2024.7976. JAMA. 2024. PMID: 38776093 No abstract available.
-
In ischemic stroke, adding IV thrombolysis ≤2 h after symptom onset to thrombectomy was associated with benefit.Ann Intern Med. 2024 Jun;177(6):JC68. doi: 10.7326/ANNALS-24-00519-JC. Epub 2024 Jun 4. Ann Intern Med. 2024. PMID: 38830216
References
-
- Turc G, Tsivgoulis G, Audebert HJ, et al. . European Stroke Organisation (ESO)-European Society for Minimally Invasive Neurological Therapy (ESMINT) expedited recommendation on indication for intravenous thrombolysis before mechanical thrombectomy in patients with acute ischemic stroke and anterior circulation large vessel occlusion. J Neurointerv Surg. 2022;14(3):209-227. doi:10.1136/neurintsurg-2021-018589 - DOI - PubMed
-
- Majoie CB, Cavalcante F, Gralla J, et al. ; IRIS Collaborators . Value of intravenous thrombolysis in endovascular treatment for large-vessel anterior circulation stroke: individual participant data meta-analysis of six randomised trials. Lancet. 2023;402(10406):965-974. doi:10.1016/S0140-6736(23)01142-X - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
