

Interobserver Reliability in the Classification of Thoracolumbar Fractures Using the AO Spine TL Injury Classification System Among 22 Clinical Experts in Spine Trauma Care
- PMID: 38324600
- PMCID: PMC10867533
- DOI: 10.1177/21925682231202371
Interobserver Reliability in the Classification of Thoracolumbar Fractures Using the AO Spine TL Injury Classification System Among 22 Clinical Experts in Spine Trauma Care
Abstract
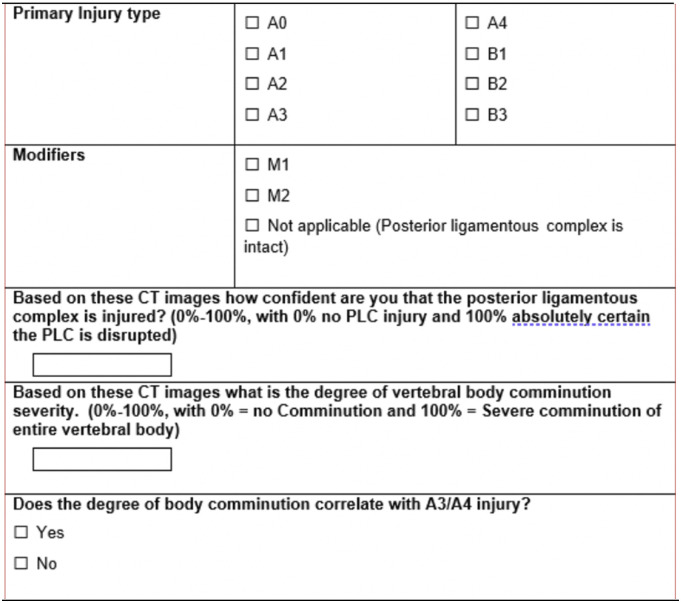
Study design: Reliability study utilizing 183 injury CT scans by 22 spine trauma experts with assessment of radiographic features, classification of injuries and treatment recommendations.
Objectives: To assess the reliability of the AOSpine TL Injury Classification System (TLICS) including the categories within the classification and the M1 modifier.
Methods: Kappa and Intraclass correlation coefficients were produced. Associations of various imaging characteristics (comminution, PLC status) and treatment recommendations were analyzed through regression analysis. Multivariable logistic regression modeling was used for making predictive algorithms.
Results: Reliability of the AO Spine TLICS at differentiating A3 and A4 injuries (N = 71) (K = .466; 95% CI .458 - .474; P < .001) demonstrated moderate agreement. Similarly, the average intraclass correlation coefficient (ICC) amongst A3 and A4 injuries was excellent (ICC = .934; 95% CI .919 - .947; P < .001) and the ICC between individual measures was moderate (ICC = .403; 95% CI .351 - .461; P < .001). The overall agreement on the utilization of the M1 modifier amongst A3 and A4 injuries was fair (K = .161; 95% CI .151 - .171; P < .001). The ICC for PLC status in A3 and A4 injuries averaged across all measures was excellent (ICC = .936; 95% CI .922 - .949; P < .001). The M1 modifier suggests respondents are nearly 40% more confident that the PLC is injured amongst all injuries. The M1 modifier was employed at a higher frequency as injuries were classified higher in the classification system.
Conclusions: The reliability of surgeons differentiating between A3 and A4 injuries in the AOSpine TLICS is substantial and the utilization of the M1 modifier occurs more frequently with higher grades in the system.
Keywords: AO spine thoracolumbar injury classification; reliability; thoracolumbar fractures.
Conflict of interest statement
Declaration of Conflicting InterestsThe author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
-
- Denis F. The three column spine and its significance in the classification of acute thoracolumbar spinal injuries. Spine. 1983;8:817. - PubMed
