

A Pilot Study of Pembrolizumab in Combination With Y90 Radioembolization in Subjects With Poor Prognosis Hepatocellular Carcinoma
- PMID: 38325328
- PMCID: PMC10911903
- DOI: 10.1093/oncolo/oyad331
A Pilot Study of Pembrolizumab in Combination With Y90 Radioembolization in Subjects With Poor Prognosis Hepatocellular Carcinoma
Abstract
Background: Combination checkpoint inhibition therapy with yttrium-90 (Y90) radioembolization represents an emerging area of interest in the treatment of advanced hepatocellular carcinoma (HCC). HCRN GI15-225 is an open-label, single-arm multicenter, pilot study (NCT03099564).
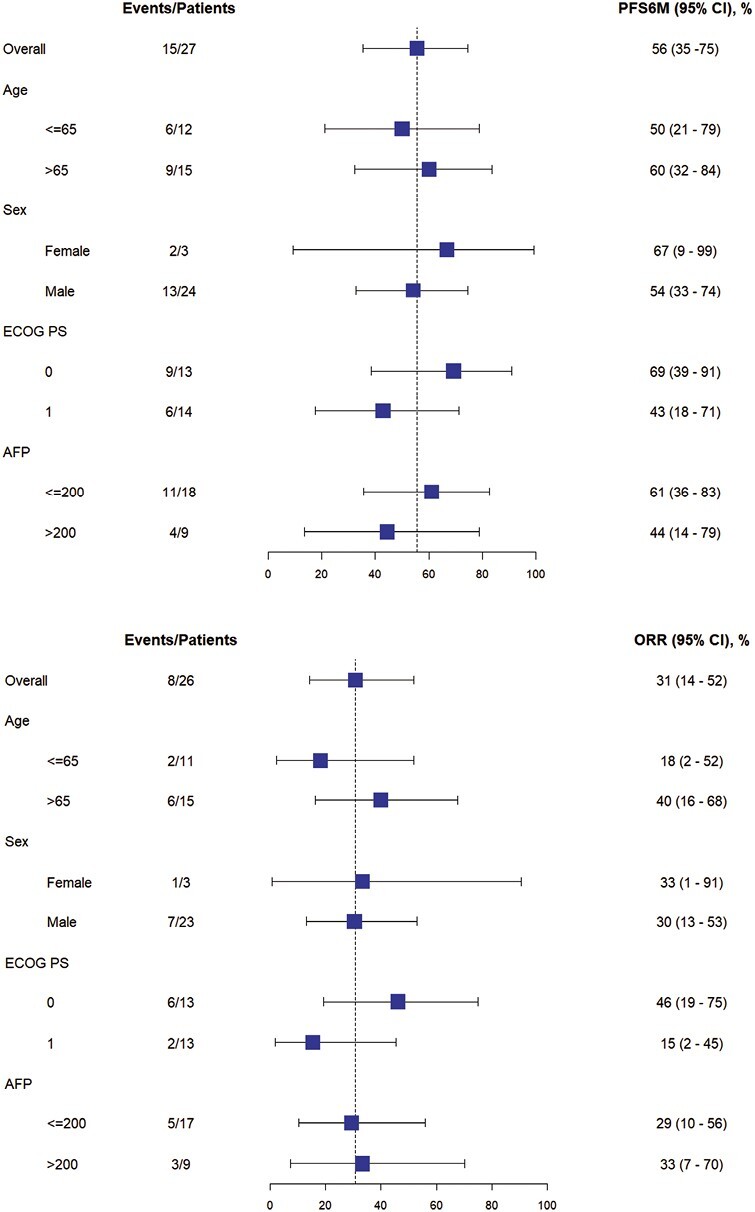
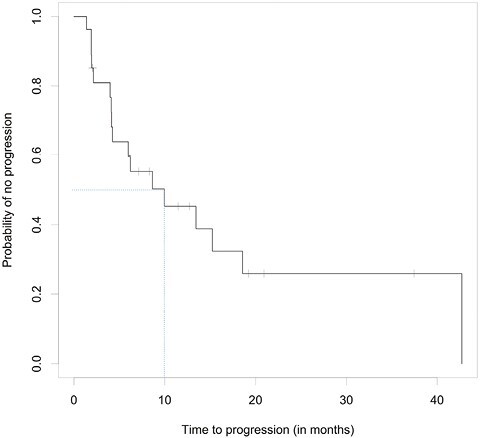
Methods: Eligible patients had poor prognosis, localized HCC defined as having portal vein thrombus, multifocal disease, and/or diffuse disease that were not eligible for liver transplant or surgical resection. Patients received pembrolizumab 200 mg intravenously every 3 weeks in conjunction with glass yttrium-90 (Y90) radioembolization TheraSphere. Primary endpoint was 6-month progression-free survival (PFS6) per RECIST 1.1. Secondary endpoints included time to progression (TTP), objective response rate (ORR), overall survival (OS), and safety/tolerability.
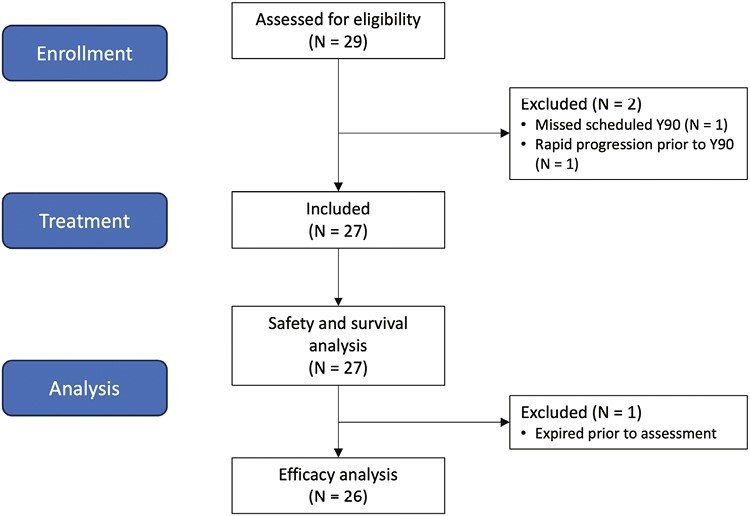
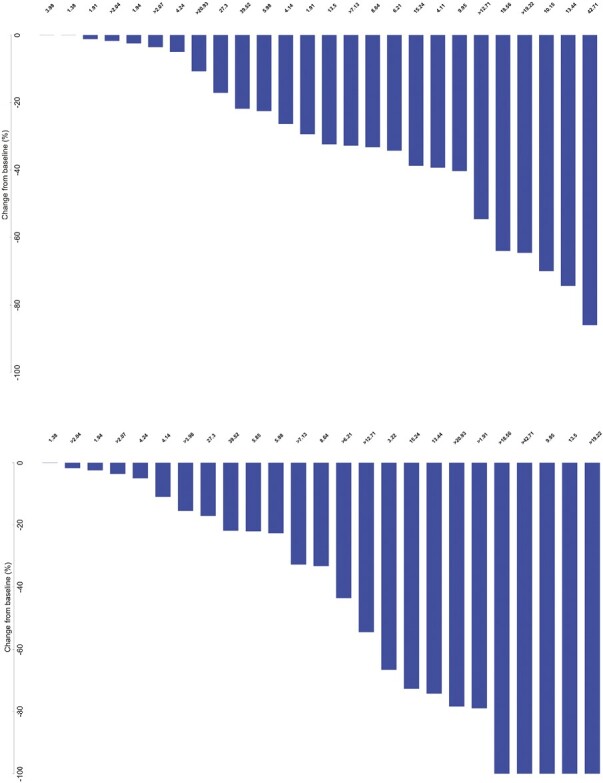
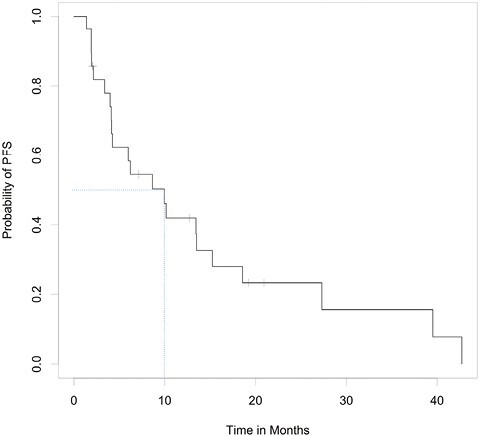
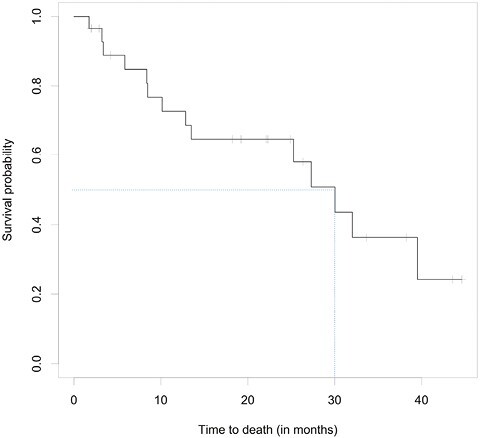
Results: Between October 23, 2017 and November 24, 2020, 29 patients were enrolled: 2 were excluded per protocol. Fifteen of the remaining 27 patients were free of progression at 6 months (55.6%; 95% CI, 35.3-74.5) with median PFS 9.95 months (95% CI, 4.14-15.24) and OS 27.30 months (95% CI, 10.15-39.52). One patient was not evaluable for response due to death; among the remaining 26 patients, ORR was 30.8% (95% CI, 14.3-51.8) and DCR was 84.6% (95% CI, 65.1-95.6).
Conclusion: In patients with localized, poor prognosis HCC, pembrolizumab in addition to glass Y90 radioembolization demonstrated promising efficacy and safety consistent with prior observations (ClinicalTrials.gov Identifier: NCT03099564; IRB Approved: 16-3255 approved July 12, 2016).
Keywords: TARE; glass Y90 radioembolization; hepatocellular carcinoma; immunotherapy; pembrolizumab.
© The Author(s) 2024. Published by Oxford University Press.
Conflict of interest statement
Shawn Yu reported ownership interests and intellectual property rights with Neoleukin Therapeutics. William P. Harris reported advisory relationships with Merck, Boston Scientific, and ICON Clinical Research; research funding (to institution) from BMS, Medimmune, Merck, Boston Scientific, Koo Foundation, Zymeworks, and Sanofi Pasteur; and expert testimony for Boston Scientific and Merck. Hanna K. Sanoff reported research funding from AstraZeneca, Merck, Bristol Myers Squibb, BioMed Valley Discoveries, Exelixis, Rgenix, Pfizer, and F Hoffman La Roche. Matthew S. Johnson is a member of the Boston Scientific Advisory Board. Ashwin Somasundaram reported a consulting/advisory relationship with Taiho. The other authors indicated no financial relationships.
Figures



References
-
- Vilgrain V, Pereira H, Assenat E, et al. ; SARAH Trial Group. Efficacy and safety of selective internal radiotherapy with yttrium-90 resin microspheres compared with sorafenib in locally advanced and inoperable hepatocellular carcinoma (SARAH): an open-label randomised controlled phase 3 trial. Lancet Oncol. 2017;18(12):1624-1636. 10.1016/S1470-2045(17)30683-6 - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
