

Oncologic outcomes of screen-detected and non-screen-detected T1 colorectal cancers
- PMID: 38325403
- PMCID: PMC11583000
- DOI: 10.1055/a-2263-2841
Oncologic outcomes of screen-detected and non-screen-detected T1 colorectal cancers
Abstract
Background: The incidence of T1 colorectal cancer (CRC) has increased with the implementation of CRC screening programs. It is unknown whether the outcomes and risk models for T1 CRC based on non-screen-detected patients can be extrapolated to screen-detected T1 CRC. This study aimed to compare the stage distribution and oncologic outcomes of T1 CRC patients within and outside the screening program.
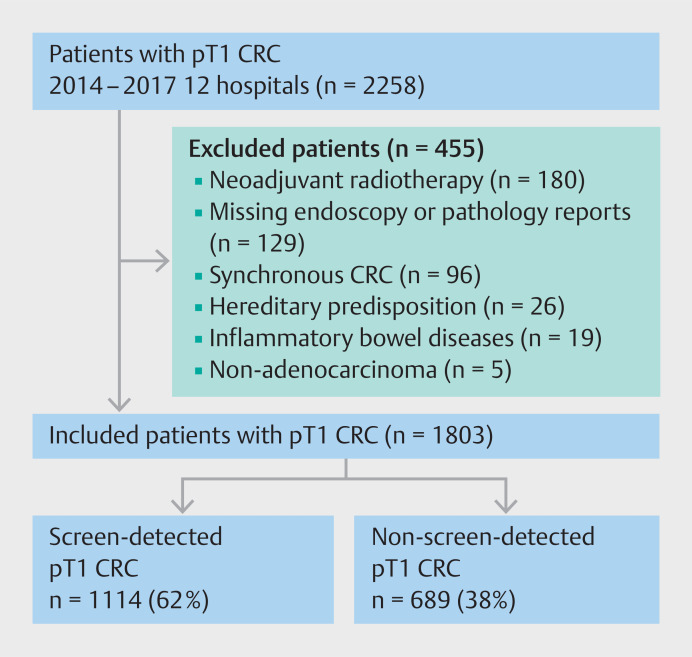
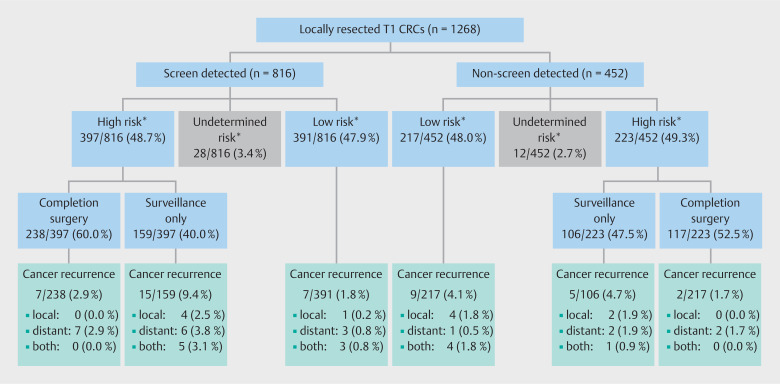
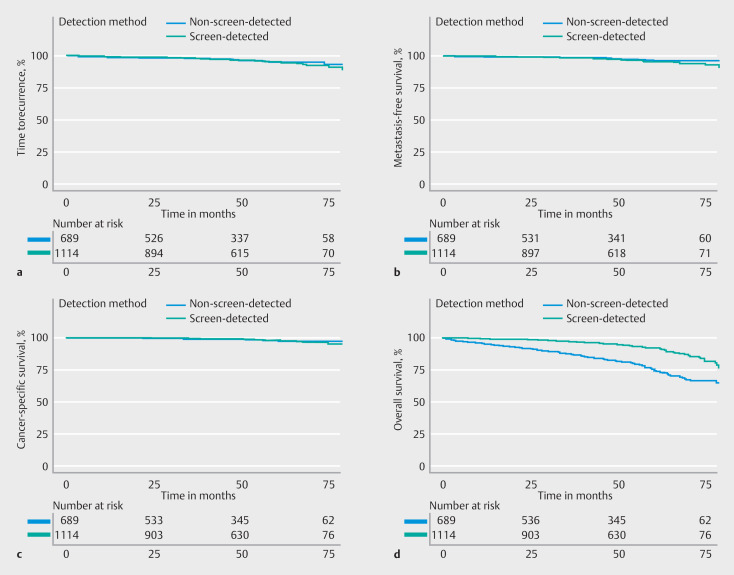
Methods: Data from T1 CRC patients diagnosed between 2014 and 2017 were collected from 12 hospitals in the Netherlands. The presence of lymph node metastasis (LNM) at diagnosis was compared between screen-detected and non-screen-detected patients using multivariable logistic regression. Cox proportional hazard regression was used to analyze differences in the time to recurrence (TTR), metastasis-free survival (MFS), cancer-specific survival (CSS), and overall survival. Additionally, the performance of conventional risk factors for LNM was evaluated across the groups.
Results: 1803 patients were included (1114 [62%] screen-detected), with median follow-up of 51 months (interquartile range 30). The proportion of LNM did not significantly differ between screen- and non-screen-detected patients (12.6% vs. 8.9%; odds ratio 1.41; 95%CI 0.89-2.23); a prediction model for LNM performed equally in both groups. The 3- and 5-year TTR, MFS, and CSS were similar for patients within and outside the screening program. However, overall survival was significantly longer in screen-detected T1 CRC patients (adjusted hazard ratio 0.51; 95%CI 0.38-0.68).
Conclusions: Screen-detected and non-screen-detected T1 CRCs have similar stage distributions and oncologic outcomes and can therefore be treated equally. However, screen-detected T1 CRC patients exhibit a lower rate of non-CRC-related mortality, resulting in longer overall survival.
The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/).
Conflict of interest statement
M. Koopman has an advisory role for Eisai, Nordic Farma, Merck-Serono, Pierre Fabre, and Servier and has received institutional grants from Bayer, Bristol Myers Squibb, Merck, Personal Genome Diagnostics (PGDx), Pierre Fabre, Roche, Sirtex, and Servier. G.R. Vink has received institutional grants from BMS, Merck, Servier, Personal Genome, Diagnostics, Bayer, Sirtex, Pierre Fabre, Lilly, and Delfi Diagnostics. F.P. Vleggaar is a consultant for Boston Scientific. L.M.G. Moons is a consultant for Boston Scientific. L. van der Schee, K.J.C. Haasnoot, S.G. Elias, K.M. Gijsbers, Y.A. Alderlieste, Y. Backes, A.-M. van Berkel, F. Boersma, F. ter Borg, E.C.H. Breekveldt, K. Kessels, I. Lansdorp-Vogelaar, M.E. van Leerdam, G. Rasschaert, R.-M. Schreuder, R.W.M. Schrauwen, T.C.J. Seerden, M.B.W.M. Spanier, J.S. Terhaar Sive Droste, E. Toes-Zoutendijk, J.B. Tuynman, W.H. de Vos tot Nederveen Cappel, and M.M. Laclé declare that they have no conflict of interest.
Figures
References
-
- Breekveldt ECH, Lansdorp-Vogelaar I, Toes-Zoutendijk E et al.Colorectal cancer incidence, mortality, tumour characteristics, and treatment before and after introduction of the faecal immunochemical testing-based screening programme in the Netherlands: a population-based study. Lancet Gastroenterol Hepatol. 2022;7:60–68. - PubMed
-
- Senore C, Giovo I, Ribaldone DG et al.Management of Pt1 tumours removed by endoscopy during colorectal cancer screening: Outcome and treatment quality indicators. Eur J Surg Oncol. 2018;44:1873–1879. - PubMed
-
- Grainville T, Bretagne J-F, Piette C et al.Management of T1 colorectal cancers detected at screening colonoscopy: A study from the French national screening programme. Dig Liver Dis. 2020;52:909–917. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous