

Persistent immune abnormalities discriminate post-COVID syndrome from convalescence
- PMID: 38326527
- PMCID: PMC11142964
- DOI: 10.1007/s15010-023-02164-y
Persistent immune abnormalities discriminate post-COVID syndrome from convalescence
Abstract
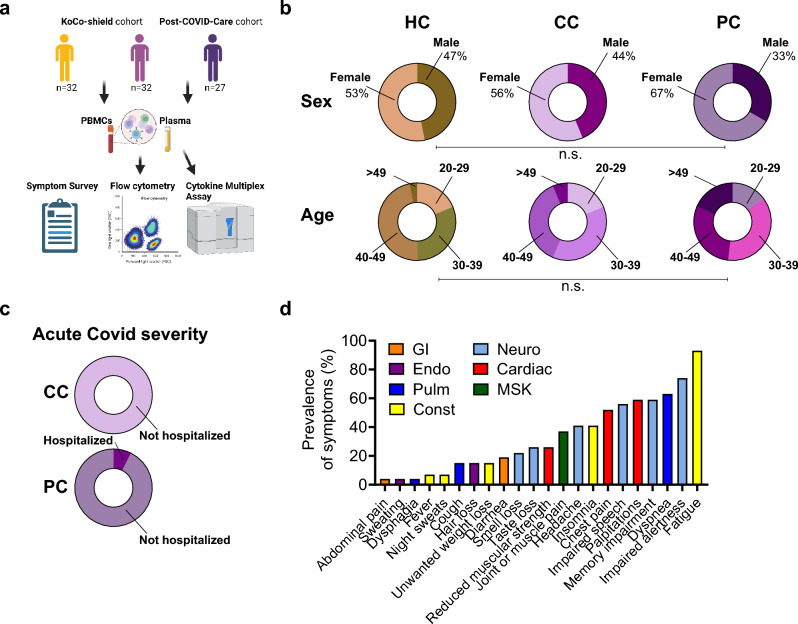
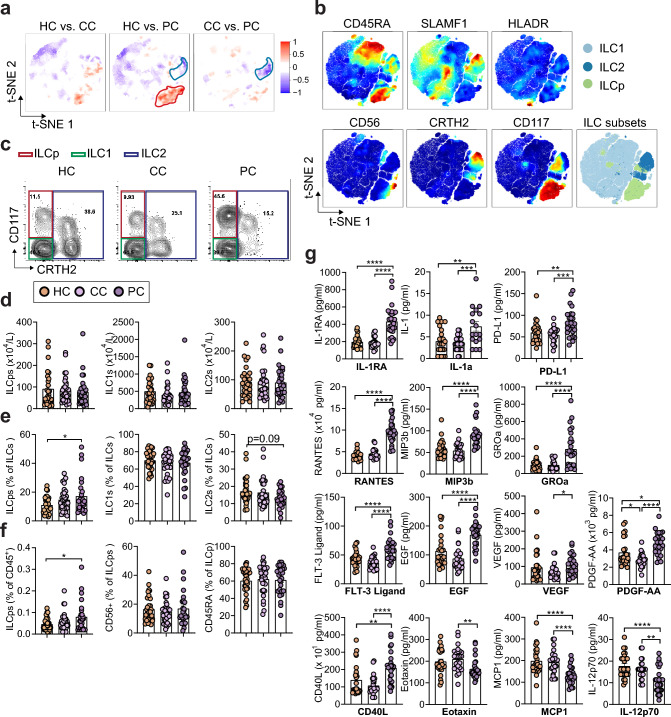
Background: Innate lymphoid cells (ILCs) are key organizers of tissue immune responses and regulate tissue development, repair, and pathology. Persistent clinical sequelae beyond 12 weeks following acute COVID-19 disease, named post-COVID syndrome (PCS), are increasingly recognized in convalescent individuals. ILCs have been associated with the severity of COVID-19 symptoms but their role in the development of PCS remains poorly defined.
Methods and results: Here, we used multiparametric immune phenotyping, finding expanded circulating ILC precursors (ILCPs) and concurrent decreased group 2 innate lymphoid cells (ILC2s) in PCS patients compared to well-matched convalescent control groups at > 3 months after infection or healthy controls. Patients with PCS showed elevated expression of chemokines and cytokines associated with trafficking of immune cells (CCL19/MIP-3b, FLT3-ligand), endothelial inflammation and repair (CXCL1, EGF, RANTES, IL-1RA, PDGF-AA).
Conclusion: These results define immunological parameters associated with PCS and might help find biomarkers and disease-relevant therapeutic strategies.
Keywords: COVID-19; Immune activation; Innate lymphoid cells; Post-COVID-19-syndrome; Tissue immunology.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no commercial or financial conflicts of interest.
Figures
References
-
- A Post-Graduate Lecture ON THE NERVOUS SEQUELÆ OF INFLUENZA. Lancet 1893;142:73–6. 10.1016/S0140-6736(00)65088-2.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
